Microsoft word - content.doc

Journal of the New Zealand Medical Association
Patients admitted with an acute coronary syndrome in New
Zealand in 2007: results of a second comprehensive
nationwide audit and a comparison with the first audit from
2002
Chris Ellis, Greg Gamble, Andrew Hamer, Michael Williams, Philip Matsis, John Elliott, Gerard Devlin, Mark Richards, Harvey White; for the New Zealand Acute Coronary Syndromes (NZACS) Audit Group
Abstract
Aims To audit all patients admitted to a New Zealand (NZ) Hospital with an acute
coronary syndrome (ACS) over a 14-day period, to assess their number, presentation
type and patient management during the hospital admission and at discharge. To
compare patient management in 2007 with the 1st NZ Cardiac Society ACS Audit
from 2002.
Methods We updated the established NZ ACS Audit group of 36 hospitals to 39
hospitals now admitting ACS patients across New Zealand. A comprehensive data
form was used to record individual patient information for all patients admitted
between 00.00 hours on 14 May 2007 to 24.00 hours on 27 May 2007.
Results 1003 patients, 9% more than in 2002 (n=930), were admitted with a
suspected or definite ACS: 8% with a ST-segment-elevation myocardial infarction
(STEMI), 41% with a non-STEMI (NSTEMI), 33% with unstable angina pectoris
(UAP), and 17% with another cardiac or medical condition. In 2007 non-invasive risk
stratification following presentation remained similar to 2002 and was suboptimal:
exercise treadmill tests (21% vs 20%, p=0.62), echocardiograms (19% vs 20%,
p=0.85). An increase in utilisation of coronary angiography was noted (32% vs 21%,
p<0.0001). In hospital revascularisation rates remained low in patients with diagnosed
ACS (n=828): STEMI (45%), NSTEMI (23%) and UAP (7.3%). In comparison to
2002, changes were noted in revascularisation techniques with percutaneous coronary
intervention (PCI) performed in 19% vs 7% (p<0.0001). The use of coronary artery
bypass grafting (CABG) remained extremely low: 2.8% vs 3.5% (p=0.20). The use of
hospital and discharge medication of proven benefit was also limited.
Conclusions A collaborative group of clinicians and nurses has performed a second
nationwide audit of ACS patients. Despite a small increase in access to cardiac
angiography, guideline recommended risk stratification following the index suspected
ACS admission with a treadmill test or cardiac angiogram occurred in only 1 in 2
(48%) patients. Furthermore, in patients with a definite ACS, levels of
revascularisation are low. (PCI 19%, CABG 2.8%). These aspects of care remain of
significant concern and have not substantially changed in 5 years. There remains an
urgent need to develop a comprehensive national strategy to improve all aspects of
ACS patient management.
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
Cardiovascular disease remains the commonest cause of death in New Zealand, being responsible for 11,293 (39%) of the 28,636 total deaths in 2004.1 Ischaemic heart disease was responsible for 6313 (22%) of these deaths. An acute coronary syndrome (ACS) is an unstable and potentially life-threatening presentation of ischaemic heart disease, and is a spectrum of clinical conditions: unstable angina pectoris (UAP), non-ST-segment elevation myocardial infarction (NSTEMI) and ST-segment elevation myocardial infarction (STEMI).
Effective treatment strategies, summarised in international2–5 and local6,7 guidelines, exist and are able to significantly improve the morbidity and mortality of this condition.
In May 2002, the Cardiac Society of New Zealand ACS Audit Group performed a comprehensive audit over a 14-day period which described patient numbers, presentation type and management during hospital admission. This audit demonstrated low levels of investigations, evidence-based treatments, and revascularisation.8 In addition, there was inequitable management as patients admitted to a hospital without cardiac interventional facilities received fewer investigations and less revascularisation than patients admitted to interventional centres.9
Significant efforts were subsequently made by clinicians to improve both the medical and invasive management of patients with ACS. Local practice consensus guidelines were written,6,7 and efforts were made to try to improve access to treatments of proven benefit.10–15 Clinicians from interventional and non-interventional centres in New Zealand aimed to facilitate the transfer of appropriate patients from Non-Interventional to Interventional hospitals: the so-called ‘hub and spoke' approach to management.16
In May 2007, the Cardiac Society of New Zealand ACS Audit Group performed a further 14-day assessment of ACS in New Zealand to record current management, to discover if significant changes had been made from 2002, and to identify areas where further improvements in service delivery may be indicated. Once again we chose to undertake the Audit during a 2-week autumn period, to be consistent with the 2002 Audit, and to minimise the known influence of seasonal change on the number of ACS patients.17
Data collection—The established ACS Audit Group network from 2002 was used, consisting of one
physician for every hospital in New Zealand that admitted ACS patients. Most centres also co-opted
one or more research nurses or registrars to assist with data collection for the study.
Since 2002, the ‘Green Lane Hospital' Cardiovascular Service in Auckland had moved to the site of the ‘Auckland Public Hospital', and these two cardiac services had combined as the ‘Auckland City Hospital' service. In addition, Waitakere Hospital in Auckland had opened a coronary care unit, and Kaitaia, Dargaville and Rawene in Northland were now actively planning to admit patients with an ACS presentation.
Other smaller hospitals in New Zealand were not actively trying to admit such patients. Therefore, in 2007 there were 39 hospitals admitting ACS patients, compared to 36 hospitals in 2002.
The data collection form recorded patient demographics, initial and discharge diagnosis, medication use in hospital and at discharge, as well as investigations undertaken and invasive treatments received by patients. The dataset collected in 2007 was similar to 2002, with additional information obtained to help assess pre-hospital presentation and aspects of PCI practice. The inclusion criterion for the audit was ‘a patient admitted overnight with a suspected or definite acute coronary syndrome'.
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
Following admission and investigations, a ‘discharge diagnosis' was subsequently determined by the local clinical team who confirmed the diagnosis of an ACS, as a STEMI, NSTEMI or UAP, or determined a ‘non-ACS' presentation resultant on investigations undertaken in hospital and the patients clinical course.
A 2-week audit period was accepted as a compromise between the need to collect sufficient patient numbers to obtain an accurate representative cohort versus the ability of mainly unfunded clinicians and nurses to collect the consecutive patient data. We collected data from 0000 hours on Monday 14 May to 2400 hours on Sunday 27 May 2007 (13–26 May in 2002).
Following input from all 39 centres, ethical approval was obtained from the Multi-region Ethics Committee. As an audit of current practice, individual patient consent was not required. The Ethics Committee permitted the collection of patient names and National Health Index (NHI) numbers to assist with accurate data collection.
Data (including revascularisation procedures) from patients subsequently transferred to another institution are ‘attributed' to their original admitting hospital. Patients readmitted within the 2 weeks have all admissions included in the data; they only represented a small percentage of the overall patient number. Ethnicity was self-reported at hospital admission.
Troponin was measured at all 39 hospitals. In May 2007 there were 11 different analysers across New Zealand provided by 5 major companies: Roche (5), Abbott (3), Bayer (1), Dade Behring (1) and Beckman Coulter (1).
In order to divide NSTEMI and UAP by means of a ‘positive' troponin18 we defined ‘normal' or ‘abnormal' troponin levels using the ‘cut-off' for ‘positive' troponins as troponin T [Roche]: ‘Modular E170', ‘Elecsys 1010', ‘Elecsys 2010', ‘COBAS 601', ‘Cardiac Reader', ≥0.03ug/L, troponin I [Abbott]: ‘Axysm' ≥0.04ug/l, troponin I [Abbott]: ‘Architect' ≥0.03ug/l, troponin I [Abbott]: ‘i-stat' ≥0.08ug/l, troponin I [Bayer]: ‘Advia centaur' ≥0.04ug/l, troponin I [Dade Behring]: ‘Dimension' ≥0.1ug/l. Hypertension and dyslipidaemia were defined as patients on treatment, or with a previous clinical diagnosis. Patients with diabetes mellitus were those on diet control, oral hypoglycaemic, or insulin treatment. Cardiogenic shock was defined as: a systolic blood pressure of <90 mmHg for at least 30 minutes, or the need for supportive measures to maintain a systolic blood pressure of ≥90 mmHg with end organ hypoperfusion.19 Sustained ventricular tachycardia was defined as >30 seconds of ventricular tachycardia, or requiring electrical cardioversion.
Statistics—Continuous data are summarised as median and interquartile range. Differences in
frequencies were tested using chi-squared procedures or Fishers exact test as appropriate. SAS (SAS
Institute Inc, v9.1) was used to perform the analyses. All tests were two-tailed and a 5% significance
level was used.
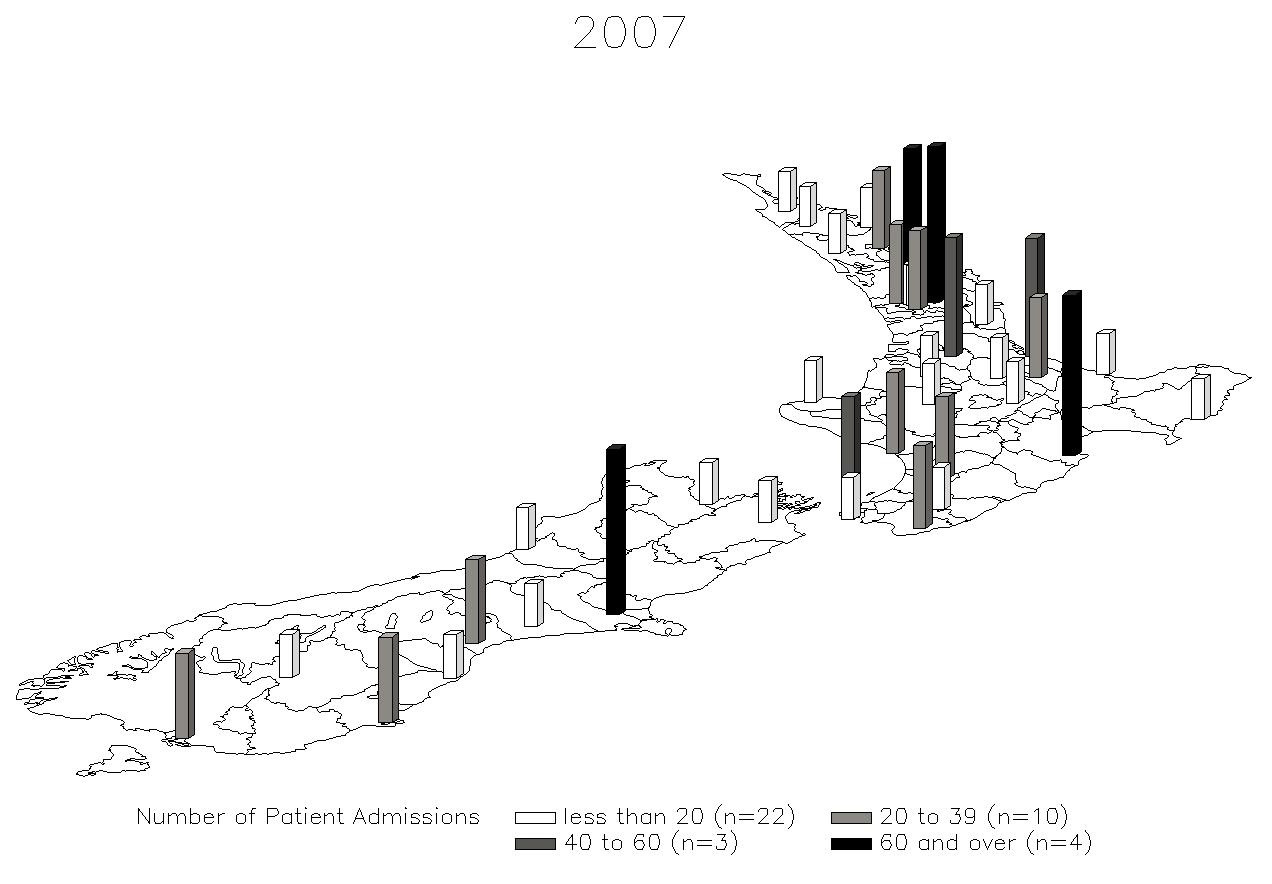
1003 patients with a suspected or definite ACS were admitted to 39 New Zealand hospitals and enrolled in the ACS audit over the 14-day period (Figure 1). Eight patients (7 once and 1 twice) were readmitted within the 2 weeks, all to the same hospital. 134 patients were transferred from their admitting hospital to another institution for further management (128 [96%] to an intervention centre). Over the 2 weeks, 3 hospitals had no ACS admissions, 8 hospitals admitted 40 or more patients of which 2 hospitals (Auckland City and Christchurch) admitted more than 120 patients, from their own catchment area.
Patient demographics: The median age was 67 (IQR 56-78) years. Forty-two percent
of patients were female, 77% Caucasian, 9.2% Maori, 3.3% Pacific Islander, 2.7%
Indian, 2.0% Asian, 0.9% from another ethnic group and in 4.8% the ethnicity was
unspecified. Patient demographics were slightly changed from those in 2002 except
that there were fewer Caucasian patients (77% vs 83%, p<0.05), more Maori (9.2% vs
6.7%, p<0.05) and more Pacific Island ethnicity patients (3.3% vs 1.5%, p<0.05) in
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
2007. In addition, more patients were now identified as being ‘dyslipidaemic' (50% vs 35%, P<0.05) and more had previously undergone CABG surgery (9.9% vs 4.6%, p<0.05) (Table 1).
Figure 1. New Zealand ACS hospitals and patient numbers: 1003 patients
admitted to 39 hospitals
Table 1. Baseline patient demographic data for 2007 (n=1003) and comparison
with the 2002 Audit baseline demographic data (n=930)
Variables
(n=1003)
Median age [years] (IQR)
Sex (male)
Ethnicity
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
Diabetes mellitus
Prior angiogram
Prior PCI
Prior CABG
Prior PVD
Prior TIA/Stroke
*P<0.05
IQR: Interquartile range; MI: Myocardial infarction; PCI: Percutaneous coronary intervention; CABG: Coronary artery bypass grafting; PVD: Peripheral vascular disease; TIA: Transient ischaemic attack; AF: Atrial fibrillation.
Patient diagnosis: Using both the admission clinical diagnosis and the measurement
of a positive troponin level, we found that 86 (9%) patients presented with a STEMI,
413 (41%) with a NSTEMI, 329 (33%) with UAP, and 175 (17%) with another
cardiac or medical diagnosis (Tables 2A, 2B, 2C, 2D). In 2007, compared with 2002,
there was a higher percentage of NSTEMI patients (413 (41%) vs 287 (31%),
P=0.0025) compared to UAP patients (Table 2B).
Patient management: 69% of STEMI patients received reperfusion therapy. The
majority received fibrinolytic therapy with only 13 (15%) of STEMI patients treated
with primary PCI. This rate had, however, increased from 2002 (13 (15%) vs 3 (3%),
p=0.0046) (Table 2A).
Table 2A. Treatments and investigations of STEMI patients: 2002 and 2007
Variables
P: 02 vs 07
101 (11%) 86 (8.6%)
Treatments in hospital
Fibrinolytic therapy
No heparin***
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
Investigations in hospital
In-hospital deaths
Discharge medications
PCI: Percutaneous coronary intervention; UF: Unfractionated; CABG: Coronary artery bypass graft; Angio: Angiogram; ETT: Exercise treadmill test; ACE: Angiotensin converting enzyme; ARB: Angiotensin receptor blocker
*** Enoxaparin or UF heparin
Overall in 2007, enoxaparin was more widely used in ACS patients than unfractionated heparin (UFH): 52% vs 5.6%, p < 0.0001. However only 339 of 752 (45%) of NSTEMI/UAP patients were treated with any heparin. Glycoprotein 2b/3a receptor blocking agents were used very rarely, in only 13 (1.6%) of ACS patients.
Cardiac investigations: Of the 1003 patient admissions, 195 (19%) underwent an
echocardiogram, 214 (21%) received an exercise treadmill test, and 317 (32%)
received a cardiac angiogram. Compared to 2002, there was no change in the
percentage of patients receiving an echocardiogram or exercise test, but more patients
in 2007 accessed cardiac angiography (317 (32%) vs 199 (21%), p<0.0001) (Table 3).
However, in 2007 of 828 ‘definite' ACS patients (STEMI, NSTEMI, UAP), half did
not undergo either non-invasive or invasive risk stratification with an exercise test or
cardiac angiography: 391 (47%) (Table 2D).
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
Table 2B. Treatments and investigations of NSTEMI patients: 2002 and 2007
Variables
P: 02 vs 07
287 (31%) 413 (41%)
Treatments in hospital
Fibrinolytic therapy
156 (54%) 271 (66%)
228 (79%) 321 (78%)
Investigations in hospital
265 (92%) 360 (87%)
180 (63%) 197 (48%)
178 (62%) 201 (49%)
In-hospital deaths
Discharge medications
228 (83%) 353 (85%)
177 (63%) 298 (72%)
127 (45%) 230 (56%)
127 (45%) 255 (62%)
153 (55%) 308 (75%)
Revascularisation: Of the 828 ‘definite' ACS patients, 291 (35%) patients underwent
a cardiac angiogram. The majority of these (62%) subsequently underwent
revascularisation prior to hospital discharge, more often using percutaneous
techniques: 157 (19%) PCI vs 23 (2.8%) CABG surgery (Table 2D). In 2007 more
‘definite' ACS patients received a cardiac angiogram (35% vs 22%, p=0.0001), and a
PCI (19% vs 6.9%, p<0.0001), but there was no increase in patients receiving CABG
surgery (2.8% vs 3.5%, p=0.20, Table 2D) compared to 2002.
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
Table 2C. Treatments and investigations of UAP patients: 2002 and 2007
Variables
P: 02 vs 07
Treatments in hospital
Fibrinolytic therapy
No heparin***
Investigations in hospital
In-hospital deaths
Discharge medications
Discharge medications: For ‘definite' ACS patients discharged in 2007 (n=815),
compared to patients discharged in 2002 (n=695), the use of aspirin and beta-blockers
was unchanged (Table 2D). However, more patients were discharged with an
angiotensin converting enzyme-inhibitor/angiotensin receptor blocker (ACE-I/ARB)
(55% vs 43%, p<0.0001), and with a statin (70% vs 55%, p<0.0001). In addition,
clopidogrel was much more frequently used for ACS patients in 2007, with 269 (33%)
of 828 patients being treated with this drug, compared to 57 (8%) of 721 patients:
p≤0.0001, in 2002.
Hospital outcomes: 16 (1.6%) patients died during their hospital admission: 5 (5.8%)
of STEMI patients, 8 (1.9%) of NSTEMI and UAP patients, and 3 (2%) of ‘other
cardiac or medical diagnosis' patients. 34 (3.4%) patients had a recurrent or
subsequent myocardial infarction, and 124 (12%) had recurrent angina. Cardiogenic
shock developed in 11(1.1%) patients. Three (0.3%) patients received an intra-aortic
balloon pump, 2 (0.2%) received a temporary pacemaker, and 4 (0.4%) patients
received a permanent pacemaker. 1 patient suffered a stroke and 19 (1.9%) sustained
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
ventricular tachycardia. Only 1.5% of patients were enrolled in a research project whilst in hospital.
Table 2D. Treatments and investigations of STEMI, NSTEMI and UAP patients
in 2002 (n=721) and in 2007 (n=828)
Variables
All "Definite' ACS Pts
P : 02 vs 07
Investigations in hospital
In-hospital deaths
Discharge Medications
721 – 26 less deaths; n=695
828 – 13 less deaths; n=815
Other lipid drug
Table 3. Investigations and revascularisation treatments in 2002 and 2007
Variables
All Patients
(n=1003)
Pulmonary oedema **
Exercise treadmill test
Cardiac angiogram
Exercise test and cardiac angiogram
Exercise test or cardiac angiogram
Neither exercise test or cardiac angiogram
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
Discussion
In a 2-week period in May 2007, 1003 New Zealanders were admitted to hospital with a suspected or definite ACS, of whom 828 patients, after investigations and review, had a final diagnosis of an ACS. If a similar number of ACS patients were admitted throughout the year, approximately 21,500 patients would present with this life-threatening illness. The optimal management of these patients is accepted and widely promulgated in local6,7 and international2–5 guidelines. As a collaborative group of clinicians we have once again collected data on the management of these patients.
Patient management
In-hospital diagnosis: The New Zealand ACS Audit group data collection is unique,
as it collects extensive data from all hospitals in one country and collects all patients
admitted within a two-week period.8,9 We identified 1003 patients admitted with
STEMI (9%), NSTEMI (41%), UAP (33%) or other cardiac or medical diagnoses
(17%). In 2007, in comparison to 2002, there was a higher percentage of NSTEMI
patients (413 (41%) vs 287 (31%), P=0.0025) (Table 2B) probably as a result of the
use of lower ‘cut off' levels for a ‘positive' troponin which had been adopted for
biochemical analysers, as compared to 2002.20 Hence more patients crossed the
‘threshold' for a ‘positive' troponin T and the diagnosis of a NSTEMI.
In-hospital investigations: For STEMI and NSTEMI (heart attack) patients (n=499),
with myocardial damage and at the highest risk, the use of guideline recommended
echocardiography (29%) and angiography (48%) was low with 43% of patients
receiving neither as a method of assessing left ventricular systolic function, an
important determinant of long-term prognosis.21
Furthermore, for the same group, the use of an exercise treadmill test (12%) or a cardiac angiogram (48%) as methods of risk assessment was also low, with 45% of patients not receiving either test. These levels of investigation contrast markedly with the recommendations of guidelines which recommend that all STEMI and NSTEMI patients be considered for assessment in these ways.
Clearly there are some patients with significant co-morbidities, in whom a non-invasive management strategy is appropriate for their care, and who would not be expected to undergo such investigations. In addition, in some patients with a recent admission when cardiac angiography did identify the coronary anatomy, further angiography may not be felt to be required. However, these issues are not unique to New Zealand patients, and to try to assess our rates, particularly of cardiac angiography, a comparison with similar studies in overseas ACS patients is warranted.
International comparisons, Europe—The most recent European Society of
Cardiology Survey22 of 3004 patients from 32 countries in 2004 demonstrated that the
rate of investigations was higher in Europe as compared to New Zealand in 2007
(Figure 2) with European STEMI patients receiving a higher rate of echocardiography
(83% vs 62%), angiography (70% vs 58%) and PCI (58% vs 45%). NSTEMI patients
in Europe, compared to patients in New Zealand, also received a higher rate of
echocardiography (72% vs 16%), angiography (63% vs 32%) and PCI (37% vs 16%).
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
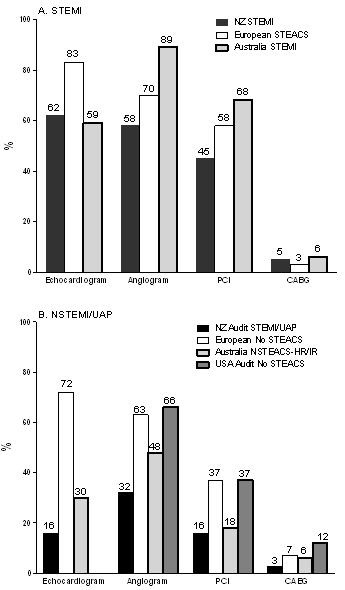
International comparisons, Australia: The Australian audit of ACS patients was
undertaken over seven months (November 2005 to May 2006) from 39 selected
hospitals across all States and territories of Australia.23 A total of 3402 patients were
enrolled: most from ‘metropolitan' centres, although ‘regional' (21% patients) and
‘rural' (3% patients) admissions were included. Australian STEMI patients receiving
a similar rate of echocardiography (59% vs 62%), more cardiac angiography (89% vs
58%) and more PCI (68% vs 45%) than New Zealand patients (Figure 2).
Figure 2. Comparison of New Zealand (2007), European (2004), Australian
(2005-2006) and USA (2002-2003) ACS patient surveys for ST-segment-elevation
ACS and No ST-segment-elevation ACS patients: investigations and
revascularisation treatments
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
Non-ST-Elevation ACS-High Risk (NSTEACS-HR) and Non-ST-Elevation ACS-Intermediate Risk (NSTEACS-IR) patients in Australia, compared to NSTEMI and UAP patients in New Zealand, also received a higher rate of echocardiography (30% vs 16%) and cardiac angiography (48% vs 32%) with a similar rate of PCI (18% vs 16%).
International comparisons, United States of America (USA)—The CRUSADE
(Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse
Outcomes with Early Implementation of the ACC/AHA Guidelines) audit from the
USA has reviewed the data from 400 participating hospitals and 43,317 high-risk
NSTEMI ACS patients with positive cardiac markers and/or ischaemic ST-segment
changes.24 NSTEMI patients in the USA, compared to patients in New Zealand
(Figure 2), received a higher rate of cardiac angiography (66% vs 32%), PCI (37% vs
16%) and CABG (12% vs 2.6%).
International comparisons, GRACE Registry—A comparison can also be made
with the 44, 372 patients enrolled in the International GRACE Registry in 2005,
which included patients from 95 hospitals in 14 countries in North and South
America, Europe, Australia and New Zealand (two sites). 25. GRACE STEMI patients
in 2005 received a higher rate of angiography (80% vs 58%) and PCI (64% vs 45%)
compared to New Zealand patients in 2007, and GRACE NSTEMI patients also
received a higher rate of angiography (63% vs 32%) and PCI (35% vs 16%).
With this high level of invasive management, STEMI patients from 1999 to 2005 in the GRACE cohort25 have shown a decline in in-hospital death (8.4% to 4.6%) and heart failure (19.5% to 11%). In addition, for NSTEMI patients from 1999 to 2005, the GRACE cohort has also been able to detect a decline in in-hospital death (2.9% to 2.2%) and heart failure (13% to 6.1%).
Medical management of NSTEMI patients—We found low levels of use of heparin
for NSTEMI patients, with 32% not accessing this treatment. In comparison, 27% of
European NSTEMI patients22 did not receive heparin, and neither did 17% of USA
patients.24 The use of a glycoprotein 2b/3a inhibitor was very low in New Zealand
NSTEMI patients with only 1.7% of patients receiving this therapy in 2007. The
numbers were also low in 2002 (2.8%). In comparison, 21% of European NSTEMI
patients22 and 35% of USA patients24 were treated with this effective strategy.
Discharge medications—The European, Australian and USA ACS patient surveys
have all shown a higher uptake of evidence-based, prognostically advantageous,
secondary prevention medication (Figure 3). The use of clopidogrel was particularly
low in New Zealand patients.
In 1996, the Clopidogrel versus Aspirin in Patients at Risk of Ischaemic Events (CAPRIE) trial26 reported that in 19, 185 patients clopidogrel was superior to aspirin over 1 to 3 years of treatment, reducing ischaemic stroke, MI, or vascular death by 8.7% (p=0.04). In 1999, Australian patients were able to access this therapy, but in New Zealand, not even patients strongly allergic to aspirin, could access funding for clopidogrel.12
Subsequent, large randomised controlled clinical trials have demonstrated the benefit of clopidogrel treatment in NSTEMI patients27, patients undergoing a coronary stent,28 and STEMI patients receiving fibrinolytic therapy.29 As a result of these and
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
other data, the European,2,3 USA4,5 and New Zealand6,7 ACS Guidelines recommend clopidogrel use for ACS patients for 9 to 12 months after presentation, and for 12 months after a coronary stent. However, from 1996 to 2007, New Zealand patients could only access clopidogrel funding [via the hospital service] for 3 weeks after a stent, and not for an ACS presentation.12
Figure 3. Comparison of New Zealand (2007), European (2004), Australian
(2005-2006) and USA (2002-2003) ACS patient surveys for ST-segment-elevation
ACS and No ST-segment-elevation ACS patients: discharge medications
Then, in October 2006, ACS patients were given limited funding for 3 to 6 months and stent patients for six months. The low numbers of patients receiving clopidogrel,
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
both in the 2002 and the 2007 Audit will have been significantly influenced by this limited funding by PHARMAC.
Most recent USA data from the ‘Get with the Guidelines' ACTION Audit—The
most recent USA Audit data comes from the American Heart Association's ‘Get with
the Guidelines (GWTG) ACTION' Audit from data collected from 1 January 2007 to
31 March 2009 from 343 sites. 46,245 STEMI and 71,536 NSTEMI patients are
represented, with 93% and 88% patients receiving a diagnostic cardiac angiogram, of
whom 89% and 55% of patients respectively received this within 24 hours of
presentation (Personal correspondence: Drs Harrington and Roe, Duke University,
USA). 72% and 42% of patients received a GP2b/3a receptor antagonist, and 90% and
86% of patients received heparin treatment, respectively.
At hospital discharge, the rates of use of proven medications for STEMI and NSTEMI patients were aspirin (98%, 97%), clopidogrel (91%, 74%), beta-blocker (97%, 95%), ACE-inhibitor/ARB (78%, 70%), and statins (92%, 86%). The clear message from this data is that with vigorous use of Guidelines and efficient hospital processes, major improvements in the use of proven medication can be achieved.
Improving quality of care
Access to investigations and treatments—Data from the second NZ ACS Audit
Group have identified limitations to the care of ACS patients in New Zealand. The
major issue in 2007 appears to be the limited availability of modern invasive
management, although with a small, but encouraging improvement from the 2002
audit. The access to CABG surgery, however, remains very limited.
In addition, the availability of non-invasive assessment tests, especially echocardiograms and exercise treadmill tests, have not improved from 2002. Further there are areas of patient management, such as the use of proven medication both within hospitals, and at hospital discharge, where significant improvements could be delivered.
Organisation of ACS services—In light of our data, one proposed solution would be
to organise National ACS services based upon a Regional strategy from each of the 5
major cardiothoracic centres30: Auckland City Hospital, Waikato Hospital, Wellington
Hospital, Christchurch Hospital and Dunedin Hospital.
An integrated approach to providing service should be considered. In particular necessary resource should be provided centrally to improve rates of angiography, PCI and CABG surgery, and to peripheral centres, for provision of echocardiography and exercise treadmill testing in particular.30 The concept of the ‘hub and spoke' approach to care of ACS patients also requires coordination of patient transfer in a timely manner, to access invasive assessment and management.31–33
Planning for acute and semi-acute transfers, similar to that already available for trauma patients in New Zealand, has the potential to markedly improve patient outcomes, and the health of many thousands of New Zealand ACS patients a year.
Governance of ACS services—There appears to be a need for Cardiologists and
Physicians in New Zealand to have a major role in the planning of ACS patient
services.30 That New Zealand's health system is subject to ‘government rather than
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
governance'32 is critically explored and discussed by respected academics: Professors Gorman and Scott from the University of Auckland, who, along with cardiologists30 have outlined the need for practicing clinicians to be a major part of health service management.
Management programmes—At a hospital level, observations among 64,775 patients
drawn from 350 USA centres showed that higher rates of adherence to guidelines
correlated with lower rates of in-hospital mortality.34 At the patient level, a clear
gradient of increasing mortality risk can be observed among patients with acute
coronary syndromes discharged on fewer evidence-based secondary prevention
therapies.
In a study of 1385 patients, being discharged on all guidelines-advocated therapies, there was a 10-fold lower risk of mortality by six months compared with the risk in those discharged on none (OR 0.10, 95% CI: 0.03–0.42; p<0.0001).35 In addition to the need for improved health promotion strategies aimed at encouraging earlier presentation to hospital, specific local programmes facilitating implementation and ongoing compliance with life-saving evidence-based therapies offer a substantial capacity to reduce mortality, and could be readily introduced to the New Zealand environment.36-40
Study limitations—As with 2002, we made significant efforts to enrol all ACS
patients into the audit. In 2002 we estimated that the number of patients ‘missed' was
4%.8 We expect that similar numbers of patients were ‘missed' in 2007; these patients
are not included nor further considered in this audit. The scope of the NZ ACS Audit
did not include an assessment of individual hospital risk tools, availability or
attendance of rehabilitation, nor more in-depth data on contra-indications for
investigations or therapies. Neither did we collect data on defibrillator device use,
nicotine patch use, or on the acute care of diabetes mellitus patients which was varied
across centres.
Conclusions
The Cardiac Society of New Zealand Acute Coronary Syndrome Audit Group has undertaken a second nationwide audit of the management of ACS patients. The audits main finding is that there are still low levels of investigations, evidence-based treatments and revascularisation undertaken for New Zealand ACS patients in comparison to overseas experiences. The reasons for this are likely to be multifactorial.
Despite some small, but encouraging increased access to angiography and subsequent revascularisation with PCI from 2002, there has been no improvement in the access to non-invasive testing. CABG surgery remains a very limited management option. There has been an increase in the use of some, but not all, proven medications. There remains a need for a comprehensive national strategy to improve all aspects of ACS patient management.
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
Competing interests: None known.
Author information: Chris Ellis, Cardiologist, Green Lane Cardiovascular Service,
Auckland City Hospital, Auckland; Greg Gamble, Statistician, University of
Auckland; Andrew Hamer, Cardiologist, Nelson Hospital, Nelson; Gerard Devlin,
Cardiologist, Waikato Hospital, Hamilton; Philip Matsis, Cardiologist, Wellington
Hospital, Wellington; John Elliott, Cardiologist, Christchurch Hospital, Christchurch;
Michael Williams, Cardiologist, Dunedin Hospital, Dunedin; Mark Richards,
Cardiologist, National Heart Foundation Professor of CVS Studies and Director of the
Cardioendocrine Research Group, University of Otago, Christchurch, Christchurch
Hospital, Christchurch; Harvey White, Cardiologist and Director of the Coronary
Care Unit & Green Lane Cardiovascular Research Unit, Green Lane Cardiovascular
Service, Auckland City Hospital, Auckland
Acknowledgements: The NZACS Audit Group is supported by small, unrestricted
educational grants from Aventis Pharmaceuticals Ltd and MSD Pharmaceuticals Ltd
who responded to an investigator initiated request to assist with data entry, statistical
and administrative support. The project was, however, entirely devised and executed
by the Steering Committee with total independence from the companies above, and
endorsed by the Cardiac Society of New Zealand, which itself made a small
contribution to costs. Collection of data was unfunded at local centres, although three
centres received a modest donation for personnel support.
We thank these audit leaders and assistants in the following hospitals—from north to south by region (patient numbers in the study are given inside brackets; #Chairman; *Steering Committee member).
Auckland/Northland (North Island)
Kaitaia Hospital: Dr E Jeffrey (9). Dargaville Hospital: Dr D Gibbons (5). Rawene
Hospital: Dr K Blattner (0). Kawakawa Hospital: Dr A Murray, Ms S August (3).
Whangarei Hospital: Dr N Harrison, Dr B Wong, Ms K O'Keefe (37). North Shore
Hospital, Auckland: Dr H Hart, Dr T Scott, Ms E Fairhurst, Ms W Young (66).
Waitakere Hospital: Dr H Hart, Dr T Scott, Ms J Hewlett (24). Auckland City
Hospital: Dr C Ellis #*, Prof H White*, Mr G Gamble*, Dr A Chateleine (122).
Mercy Private Hospital, Auckland: Dr C Ellis, Ms C McGarrigle (6). Ascot Private
Hospital, Auckland: Dr A Maslowski (2). Middlemore Hospital, Auckland: Dr A
Kerr, Dr M Lund, Dr J Goh (35).
Waikato (Central North Island)
Thames Hospital: Dr J Lennane, Dr Aftabuzzaman (19). Tauranga Hospital: Dr J
Tisch, Dr G Porter, Dr C Young, Ms W Bryson, Ms J Goodson (44). Waikato
Hospital, Hamilton: Dr G Devlin*, Ms B Killion, Ms A Silverstone, Ms L Boenders
(56). Whakatane Hospital: Dr E Edwards, Dr R Steeper, Ms D Garner (12).
Rotorua Hospital: Dr N Crook, Ms A Morley (28). Tokoroa Hospital: Dr N
Thornton, Dr F Kanan (2). Te Kuiti Hospital: Dr N Thornton, Dr K Buswell, Ms T
Te Wano (0). Taupo Hospital: Dr K Logan (11). Gisborne Hospital: Dr C Duffy,
Ms K Weytmans, Ms T Low (16). Taumarunui Hospital: Dr N Thornton, Dr H
Wahid (1). New Plymouth Hospital: Dr I Ternouth, Dr T Boswell (17).
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
Wellington (Southern North Island, Upper South Island)
Hawkes Bay Regional Hospital, Hastings: Dr R Luke, Ms J MacKenzie (76).
Wanganui Hospital: Dr T Thompson, (26). Palmerston North Hospital: Dr D Tang
(25). Masterton Hospital: Dr T Matthews, Ms K Lee (10). Hutt Hospital: Dr T
O'Meeghan, Ms J Dewar, Ms M Klientjes (25). Wellington Hospital: Dr P Matsis*,
Ms D Middleditch, Ms E Walsh (57). Wakefield Private Hospital, Wellington: Dr
M Abernethy (0). Nelson Hospital: Dr A Hamer, Ms R Price (14). Blenheim
Hospital: Dr M Heynike, Ms M Udy (12).
Christchurch/Canterbury (Central South Island)
Greymouth Hospital: Dr U Bopitiya, Ms L Skeats (6). Christchurch Hospital:
Assoc Prof J Elliott*, Prof M Richards*, Ms L Skelton, Ms L Frost (141). Ashburton
Hospital: Dr A Obafemi, Ms A Smart (3). Timaru Hospital: Dr M Hills, Ms Maria
Hammond, Ms C Barker (31).
Dunedin/Otago (Southern South Island)
Oamaru Hospital: Dr D Phillips, Ms S McCulloch (10). Dunstan Hospital, Clyde:
Dr G Nixon, Ms J Coutts (3). Dunedin Hospital: Assoc Prof MJA Williams*, Ms M
McLelland (28). Invercargill Hospital: Dr A Maloney, Dr R Anand (21).
Correspondence: Dr Chris Ellis, Chairman of the NZACS Audit Group, Cardiology
Department, Green Lane CVS Services, Level 3, Auckland City Hospital, Grafton,
Auckland 1023, New Zealand. Email: [email protected]
References:
1. New Zealand Health Information Service. Mortality and demographic Data 2004.
2. Bassand J, Hamm CW, Ardissino D, et al. Guidelines for the diagnosis and treatment of non-
ST-segment elevation acute coronary syndromes: The Task Force for the Diagnosis and Treatment of Non-ST-Segment Elevation Acute Coronary Syndromes of the European Society of cardiology. Eur Heart J 2007;28:1598-1660.
3. Van de Werf F, Bax J, Betriu A et al. Management of acute myocardial infarction in patients
presenting with persistent ST-segment elevation: The Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of cardiology. Eur Heart J 2008;29:2909-2945.
4. Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 Guidelines for the
Management of Patients with Unstable Angina/Non ST-Elevation Myocardial Infarction Executive Summary. J Am Coll Cardiol 2007;50:652-726.
5. Antman EM, Hand M, Armstrong PW et al. 2007 Focused Update of the ACC/AHA 2004
Guidelines for the Management of Patients with ST-Elevation Myocardial Infarction. J Am Coll Cardiol 2008;51:210-247.
6. Non ST-Elevation Acute Coronary Syndrome Guidelines Group and the New Zealand Branch
of the Cardiac Society of Australia and New Zealand. Non ST-elevation myocardial infarction: New Zealand management guidelines. NZ Med J 2005;118:1-19. http://www.nzma.org.nz/journal/118-1223/1680
7. ST-Elevation Acute Coronary Syndrome Guidelines Group and the New Zealand Branch of
the Cardiac Society of Australia and New Zealand. ST-elevation myocardial infarction: New Zealand management guidelines. NZ Med J 2005;118 (1223). http://www.nzma.org.nz/journal/118-1223/1679
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
8. Ellis C, Gamble G, French J et al. Management of patients admitted with an Acute Coronary
Syndrome in New Zealand: Results of a comprehensive nationwide audit. NZ Med J 2004;117(1197). http://www.nzma.org.nz/journal/117-1197/953
9. Ellis C, Devlin G, Matsis P, et al. Acute Coronary Syndrome patients in New Zealand receive
less invasive management when admitted to hospitals without invasive facilities. NZ Med J. 2004;117(1197). http://www.nzma.org.nz/journal/117-1197/954
10. Elliott J, Richards M. Heart attacks and unstable angina (acute coronary syndromes) have
doubled in New Zealand since 1989: how do we best manage the epidemic? NZ Med J 2005;118(1223). http://www.nzmj.com/journal/118-1223/1674
11. Devlin G, Anderson FA, Heald S, et al. Management and outcomes of lower risk patients
presenting with acute coronary syndromes in a multinational observational registry. Heart 2005; doi: 10.1136/hrt.2004.054007.
12. White H, Ellis C. PHARMAC and lack of funding for clopidogrel. NZ Med J 2006;119(1228).
13. Ellis C, White H. PHARMAC and the statin debacle. NZ Med J 2006;119(1236).
14. Tang WT, Wong C, Herbison P. Community hospital versus tertiary hospital comparison in
the treatment and outcome of patients with acute coronary syndrome: a New Zealand experience. NZ Med J 2006;119:1238. http://www.nzma.org.nz/journal/119-1238/2078
15. Williams M. Percutaneous coronary intervention in New Zealand. NZ Med J 2007;120:1248.
16. White HD. Systems of care. Need for hub-and-spoke systems for both primary and systematic
percutaneous coronary intervention after fribrinolysis. Circulation 2008;118:219-222.
17. Ellis CJ, Gamble GD. Seasonal influence on death from ischaemic heart disease: Data from
the Southern hemisphere. NZ Med J 2002;115(1162). http://www.nzma.org.nz/journal/115-1162/194
18. Thygesen K, Alpert JS, White HD, on behalf of the Joint ESC/ACCF/AHA/WHF Task Force
for the Redefinition of Myocardial Infarction. J Am Coll Cardiol 2007;50:2173-2195.
19. Hockman JS, Sleeper LA, Webb JG, et al. Early revascularisation in acute myocardial
infarction complicated by cardiogenic shock. N Eng J Med 1999;341:625-634.
20. Latif M, Chataline A, Gamble G, et al Different analysers and variable thresholds with
troponin testing in New Zealand 2002-2007: is it time for some National standardization? Heart Lung and Circulation 2008;17(2):15.
21. Boden WE, Eagle K, Granger CB. Reperfusion strategies in acute ST-segment elevation
myocardial infarction. A comprehensive review of contemporary management options. J Am Coll Cardiol 2007;50:917-929.
22. Mandelzweig L, Battler A, Boyko V, et al. The second Euro Heart Survey on acute coronary
syndromes: characteristics, treatment, and outcome of patients with ACS in Europe and the Mediterranean Basin in 2004. Eur Heart J 2006;27:2285-2293.
23. Chew D, Amerena J, Coverdale S, et al. Current management of acute coronary syndromes in
Australia: observations from the acute coronary syndromes prospective audit. Int Med J 2007;37:741-748.
24. Sonel AF, Good CB, Mulgund J, et al. Racial variations in treatment and outcomes of black
and white patients with high-risk non-ST-Elevation acute coronary syndromes. Insights from CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines). Circ 2005;111:1225-1232.
25. Fox KAA, Steg PG, Eagle KA, et al. Decline in rates of death and heart failure in acute
coronary syndromes, 1999-2006. JAMA 2007;297 1892-1900.
26. CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in
patients at risk of ischaemic events (CAPRIE). Lancet 1996;348:1329-1339.
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
27. Yusuf S, Zhao F, Mehta SR, et al. Effects of clopidogrel in addition to aspirin in patients with
acute coronary syndromes without ST-segment elevation. N Engl J Med. 2001:345:528-532.
28. Steinhubl SR, Berger PB, Mann JT, et al. Early and sustained dual oral antiplatelet therapy
following percutaneous coronary intervention: A randomized controlled trial. JAMA. 2002;288:2411-20.
29. Sabatine MS, Cannon CP, Gibson CM, et al. Addition of clopidogrel to aspirin and
fibrinolytic therapy for myocardial infarction with ST-segment elevation. N Eng J Med. 2005;352:1179-1189.
30. Ellis CJ, Hamer AW. Cardiovascular health in New Zealand: areas of concern and targets for
improvement in 2008 and beyond. NZ Med J 2008;121(1269):5-10. http://www.nzma.org.nz/journal/121-1269/2927
31. White HD, Chew DP. Acute myocardial infarction. Lancet 2008;372:570-584. 32. Gorman D, Scott J. New Zealand's health system is subject to government rather than
governance: inadequate representation of doctors in the health system elite. NZ Med J 2008;121(1276). http://www.nzma.org.nz/journal/121-1276/3113
33. Wong C, Tang EW, Herbison P. Survival over 5 years in the initial hospital survivors with
acute coronary syndrome: a comparison between a community hospital and a tertiary hospital in New Zealand. NZ Med J 2007;120(1261). http://www.nzma.org.nz/journal/120-1261/2713
34. Peterson ED, Roe MT, Mulgund J, et al. Association between hospital process performance
and outcomes among patients with acute coronary syndromes. JAMA 2006;295:1912-1920.
35. Mukherjee D, Fang J, Chetcuti S, et al. Impact of combination evidence-based medical
therapy on mortality in patients with acute coronary syndromes. Circulation 2004;109:745-749.
36. Chew D, White HD. Myocardial Infarction Mortality-Where do we go now? European
Cardiovascular Disease 2007; Issue 1:33-34.
37. Carlhed R, Bojestig M, Wallentin L, et al. Improved adherence to Swedish national guidelines
for acute myocardial infarction: the Quality Improvement in Coronary Care (QUICC) study. Am Heart J 2006;152:1175-1181.
38. Mark DB, Van de Werf FJ, Simes RJ, et al. Cardiovascular disease on a global scale: defining
the path forward for research and practice. Eur Heart J 2007;28:2678-2684.
39. Schiele F, Meneveau N, Seronde MF, et al. Compliance with guidelines and 1-year mortality
in patients with acute myocardial infarction: a prospective study. Eur Heart Journal 2005;26:873-880.
40. Scott IA, Denaro CP, Hickey AC, et al. Optimising care of acute coronary syndromes in three
Australian hospitals. Int J of Quality in Health Care 2004;4:275-284.
NZMJ 30 July 2010, Vol 123 No 1319; ISSN 1175 8716
Source: http://www.iccnetsa.org.au/Data/Sites/1/news/2010_ellisetal.pdf
J. Technol. Manag. Innov. 2016. Volume 11, Issue 1 Unpacking ‘Give Back Box:' A Social Enterprise at the Intersection of Leadership, Innovation, and Sustainability Eduardo Barrientos 1*, Anne H. Reil y 1 Abstract: Once the domain of government agencies and non-profit organizations, a social enterprise integrates social benefits such as employment
TEIL I · Die Depression TEIL II · Die Homöopathie: Eine wirkungsvolle Lösung 5. Was ist Homöopathie und wie funktioniert sie? . . . . .346. Eine sehr persönliche Medizin. . . . . . . . . . . . .477. Homöopathie bei Depressionen?. . . . . . . . . . . .528. Was unterscheidet die Homöopathie von den konventionellen Ansätzen? . . . . . . . . . . . . . .56