Microsoft word - new hair restoration ebook.doc
Hair Transplants
Dr Jennifer Martinick
www.martinick.com
Acknowledgements: My present level of understanding, insight and know how into the hair loss industry is due to the willingness of many talented members of the Interna-tional Society of Hair Restoration Surgery (ISHRS) freely sharing their experience and knowledge with their colleagues. This book reflects some of the key fundamental work developed and per-formed by them over the past two decades. I thank all those pioneers, ca-pable path finder's who allowed me to combine most of their findings and conclusions which enabled me to make to this branch of medicine, a small contribution to the existing total knowledge. Hopefully this book will assist with the sharing of this information with the general public. Copyright 2009 Dr Jennifer Martinick, MBBS FACCS Australia/New Zea-land Without limiting the rights under copyright above, no part of this publica-tion may be reproduced, stored in or introduced into a retrieval system, or transmitted, in any form, or by any means (electronic, mechanical, photo-copying, recording, or otherwise), without the prior written permission of publisher of this book.
Cover: Art design by Micah Harmon ISBN 978-0-646-50687-6 Medical Disclaimer The purpose of this book is to provide the public with general information on hair restoration. Information provided should not be used for medical diagnosis and/or treatment.

Dr Jennifer Martinick displaying her Platinum Follicle Award
that indicates superior achievement in hair transplant surgery.

Dr Martinick showing patient hair image with mirror.

Sixth year medical student is assisting with ongoing research
into improving hair transplanting techniques and outcomes.


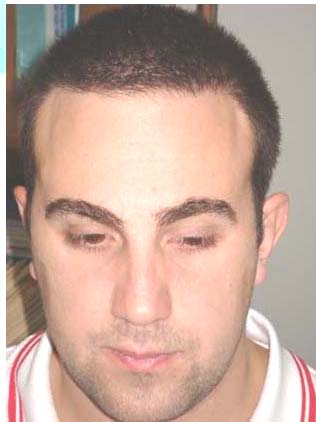
The new hair line restoration is natural and undetectable
following a 1000 graft follicular unit transplant.

Powerful operating microscopes allow skilled technicians to see
each individual follicle during graft preparation.
Table of Contents
1 New Follicular Hair Transplant . 1
2 Methods of Halting Hair Loss . 13
3 Best Hair Transplant Surgery . 29
4 Hair Restoration Consultation . 41
5 The Medical Evaluation . 49
6 Follicular Unit Extraction. 55
7 Preparing for Surgery . 59
8 Hair Restoration Procedure. 67
9 Women's Hair Loss . 91
10 Repairing Superseded Techniques . 101
11 Eyebrows and Eyelashes . 105
12 Summary. 107
13 Hair Transplantation Q&A . 109
Reference/Notes . 123
Additional Information. 125
1 New Follicular Hair Transplant
dvances in medical research, technology and surgical
Atechniques have renewed public faith in medical hair res-
toration. Using the Multi-Therapy combination we now have the means to stop or reverse hair loss.
In addition, significant advances in Hair Transplant
techniques can now offer completely natural and undetectable outcomes. This is called Follicular Unit Transplant (FUT) which is now offered as part of the Multi-Therapy approach. This is an exciting new solution that has given new life and excellent results to thousands of people.
When you experience hair loss, the resultant premature
ageing may lead to lower self esteem. Each day your self-
image is reflected in the mirror and the disparity may begin to
cause concern. Most men and women instinctively have the
desire to look and feel good, and a western culture model
promotes a fresh, youthful look¹. Technological advances in
medicine have improved the results of cosmetic surgery and
have led to an increase in popular demand.
The Role of Surgical Hair Restoration
Surgical hair restoration (also known as hair transplantation)
promotes re-growth of hair in areas affected by hair thinning
and loss. Medical research2 shows that not all hairs are created
equal. Even at advanced stages of hair loss, most men retain a
ring of hair around the sides and back of their heads. This hair
is different genetically from hair located at the hairline and top
of the scalp.

2 New Hair Restoration
In hair transplant surgery, doctors take, or ‘harvest',
permanent hair follicles from a strip of the scalp removed from the back of the head. The strip contains hundreds, usu-ally thousands of grafts, each consisting of a few hairs that can be surgically placed for growth in otherwise bald spots. This hair transplanted to bald areas will grow as well as it did in the harvested ‘donor' areas and will continue to grow perma-nently.
In order to stop and reverse the hair loss process, pa-
tients often require a Multi-Therapy approach. In these cases, doctors commonly prescribe one; two or all three United States Food and Drug Administration (FDA) approved medi-cal therapies, Rogaine®, Propecia®, or the HairMax Laser-Comb®, as well as a transplant.
Immediately after surgery Just one session of grafting
New Follicular Hair Transplant 3
Hair Plugs Are Out Follicular Units Are In!
Unfortunately, when most people think of hair replacement,
they visualize the artificial image of a doll's head. For many
years transplants were performed using large groupings or
"plugs" of hair (tufts of as many as thirty hairs) into a patient's
frontal hairline and on top of the scalp. The result looked un-
natural and was always easy to spot.
The "pluggy" transplant performed over a decade earlier shows
the "corn row" appearance that was used in transplant surgery.
As surgical hair restoration has evolved, so have the
outstanding results that skilled physicians can deliver to their patients. Follicular Unit Transplant is the new standard of hair replacement that allows surgeons to recreate the natural hair-line. With this technique, surgeons can place Micro Grafts containing one to four hairs into the recipient sites to achieve a more natural appearance. Careful orientation of the follicles so that they follow the natural direction of the hair, and taking care to place them so they do not overlap or line up unneces-sarily, helps to achieve maximum coverage. These directions are known as coronal versus sagittal placements.
4 New Hair Restoration
Note the individual hairs in what had been a balding head.
New Follicular Hair Transplant 5
Not seeking a full head of hair, merely a pleasing, fuller hairline,
this patient achieved his desired look.
6 New Hair Restoration
Before and after
Follicular Unit
Transplant.
New Follicular Hair Transplant 7
Patient before and immediately after surgery.
8 New Hair Restoration
Same patient six months after hair transplant surgery.
New Follicular Hair Transplant 9
The same patient twelve months after surgery.
10 New Hair Restoration
The Newer Surgical Techniques Demand Skilled
Surgeons
Older techniques and technology significantly hindered sur-
geons' abilities to give their hair transplant patients aestheti-
cally natural-looking hairlines. The Follicular Unit Transplant
technique opens the way to master the technology and fine art
of hairline design known as the ‘snail track'. This new tech-
nique earns its name from the way it mimics the natural hair
line irregularity, ruling out a sharply defined edge. It is also
denser in some parts - a feature of youthful hairlines.
Aided by powerful microscopes and better surgical in-
strumentation, surgeons today have the tools to create re-markably natural hairline results for patients. The best hair restoration surgeons also possess the skills needed to design the micro-elements of the hairline at the transplant recipient site. This is where size of the site, angulation, orientation and spacing are specifically and artistically determined. These sur-gical and aesthetic skills ultimately determine how the hair will grow into outstanding, newly re-created hairlines.
A Brief Comparison of New and Old Surgical
Methods
To appreciate the significance of the advances that have been
made towards evolution in these marvellous modern proce-
dures, here is a summary of the more popular older tech-
niques:
Reduction - This surgical procedure removed bald skin from
the top of the head, thereby reducing the size of area requiring
transplanted hair. Scalp reductions peaked in popularity in the
mid-1990's. Fewer of these procedures are being performed
because of various complications. These include stretching
back of the balding area, the potential for visible scarring with
New Follicular Hair Transplant 11
progressive hair loss, thinning of the donor area hair density and the popularity of new grafting techniques. Flap Surgery – The main benefit of this procedure has been its ability to cover large areas quickly. However, it involves cut-ting out a section of the bald scalp and lifting off a flap of hair-bearing skin still attached at one end. This hair-bearing flap, connected to the original blood supply, is then moved into position and sewn into place. In addition to being painful, this procedure often produced severe scarring and an unnatural appearance due to abnormal orientation of hair growth. The recovery period was longer and patients experienced more dis-comfort with this procedure. In the hands of less experienced surgeons, it often produced poor results. Mini Graft Hair Transplants – This method of hair transplan-tation was popular 10 to 15 years prior to Follicular Unit graft-ing and the follicular Micro Grafting techniques. It offered significant improvement over the old method of taking 10 to 15 hair "plugs" from the back of the head and inserting them into round holes in the bald scalp. As mentioned, these rela-tively large grafts were placed into large slits in the scalp with significant spacing between them. This technique replaced the even larger, unacceptable plugs of hair that were commonly used and represented an important step in the evolution that has led to the techniques performed today. In spite of the exis-tence of the newer methods, there still are surgeons who con-tinue to perform Mini Graft hair transplantation procedures.
12 New Hair Restoration
The Very Latest Method
There is no doubt that the new Follicular Unit Transplant of-
fers the most advanced hair replacement in hair transplant sur-
gery. It requires greater skill on the part of the surgeon and
surgical team, as well as additional time to complete. In my
experience, implanting hair follicles coronally (so that each
individual hair can be seen) achieves greater coverage than
hair follicles implanted sagittally (where the hairs lie on top of
one another, giving the appearance of less hair). A Follicular
Hair Transplant is far more attractive and with good surgical
skill to give correct orientation, is impossible to distinguish
from a person's natural hair growth on the remaining part of
the scalp. For someone seeking attractive, natural-looking
hair, this is the new procedure.
2 Methods of Halting Hair Loss
he Multi-Therapy approach requires a hair restoration
T surgeon who can demonstrate expertise using the latest
proven approaches to hair restoration.
The Multi-Therapy Approach to Hair Restoration
– Taking Control of Hair Loss
This consists of surgical grafts and FDA approved medication
or therapy.
It is important to understand that surgical hair replace-
ment without adjunctive medical therapy may not be adequate to provide the best results. There are only three FDA approved therapies for treatment of hair loss besides a surgical hair transplant:
(i) Minoxidil (Rogaine®) is a topical lotion applied to
the scalp daily. Available over-the-counter in 2% or 5% solu-tion, it is often only effective for approximately 2 years. Its exact mode of action is unknown, but it is thought to promote hair growth by increasing blood circulation locally.
(ii) Finasteride (Propecia®) is a tablet taken daily, and
acts by inhibiting the conversion of testosterone to dihydrotes-tosterone (DHT), which is the cause of male pattern hair loss. Available only on prescription, it can not be taken by women.
14 New Hair Restoration
Propecia® slows hair loss and stimulates some new hair growth, and works more effectively on the crown and mid-scalp than the frontal area. It may be prescribed in addition to a transplant to prevent further loss.
(iii) The most recently approved treatment uses low
level red laser light (655nm) which stimulates hair follicles. The size of a normal hairbrush, the HairMax LaserComb® is used twice a week. It improves the strength and appearance of hair as well as hair growth.
If a physician does not offer appropriate medical
therapies or treatments in conjunction with surgery to stop the progression of future hair loss and to enhance the quality of the remaining hair, additional surgical transplant sessions may be required.
After medical evaluation and consultation with a new
patient, your surgeon will determine the treatment plan most suitable for the individual. It must be safe, realistic and ac-complish appropriate hair restoration objectives. This is the goal.
Many patients are amazed with the hair restoration re-
sults when the work is performed by a qualified, skilled hair surgeon. The Multi-Therapy approach is highly recommended by hair restoration surgeons who are in the forefront of their profession maximising results, patient care and comfort.
Find a Qualified Hair Restoration Surgeon
There are several thousand hair restoration surgeons world-
wide who practise hair restoration. Only a small percentage
practise full time hair transplantation. In Australia there are 13
full and part time doctors who conduct hair transplant surgery.
In the United States, physicians who are licensed as medical
doctors (MD and DO) are approved to perform surgical hair
restoration regardless of any special training in this field. The
Methods of Halting Hair Loss 15
vast majority of hair restoration surgeons have also trained in dermatology, cosmetic and plastic surgery.
Within this highly specialised field, the leading sur-
geons bring outstanding education, training, skills and phi-losophy into their practices. Many of the top hair restoration practitioners are members of the International Society of Hair Restoration Surgery (ISHRS), and, in Australia, the Austral-asian Society of Hair Restoration Surgery (ASHRS).
To treat hair loss, it is critical to find a qualified hair
restoration surgeon with expertise in the Multi-Therapy ap-proach. They need to be experienced in the latest surgical techniques as outlined in these chapters.
One of the best ways to evaluate hair restoration sur-
geons is to meet and talk with several of the doctors' patients who have had hair transplants. As you interview each patient seek answers to these questions.
• How many surgical procedures have you under-
gone (and how long ago)?
• May I see pictures of how you looked before?
• How many grafts have been transplanted?
• Examine the hairline and donor site. (Have the pa-
tient comb the hair back and off of the hairline).
• What medical treatments and therapies have you
tried and what are you currently using?
• Were you comfortable during the procedure?
• How satisfied are you with the results of your hair
restoration? Did it meet your expectations?
• How accurate was the information the doctor pre-
sented regarding what would be required to meet your hair restoration objectives?
• How did you choose the doctor?
• How would you describe your overall experience?
• Did the doctor and the clinic deliver as promised?
16 New Hair Restoration
Do Your Homework
As you continue reading, you will become acquainted with the
most widely accepted components in use by skilled hair sur-
geons who offer current Multi-Therapy approach to hair resto-
ration. You will also be encouraged to further research each of
these options before undergoing any hair restoration treatment.
In addition to reading the latest information written by
respected hair restoration surgeons and authorities, you will find the following Internet websites to be reputable sources of current information:
• International Society of Hair Restoration Surgery
• International Alliance of Hair Restoration Sur-
geons (www.iahrs.org )
• Hair Loss Information – Balding Blog (www.baldingblog.com ) • Hair Loss Help (www.hairlosshelp.com )
• Hair Loss Info (www.hairlossinfo.com.au )
If you are interested in learning more about the specific medi-cal therapies discussed in each of the following sections, read the FDA approved product literature for Rogaine®, Propecia® and HairMax LaserComb® that is available on their websites:
• www.rogaine.com
• www.propecia.com
• www.lasercomb.net
A word of caution: There are thousands of websites,
message boards and chat rooms that promote unreliable and unproven advice and remedies for hair growth. Don't be mis-led.
Methods of Halting Hair Loss 17
Another prospective medical therapy is Dutasteride. This drug
is still in clinical trials for use in treatment of hair loss and
awaits FDA approval.
Make Sure the Hair Loss Treatment is
FDA- Approved
There are many so-called hair loss "remedies" on the market.
Their various claims include the use of all-natural substances
and nothing short of miraculous hair growth. Such products
often offer a "money-back guarantee" as part of their radio,
television, newspaper or Internet pitch. If it sounds too good to
be true, then it probably is.
Although some of the products advertised may thicken
hair to some degree, none have passed rigid FDA testing. Generally such products are ineffective in treating hair loss. You may even lose more of your valuable hair, time and money, waiting for these products to bear results.
If you suffer from hair loss and want to try non-surgical
hair restoration treatments first, make sure you research proven methods.
Rogaine® (Minoxidil 5% solution) and Propecia® (Fi-
nasteride 1 mg) are the only medications that have passed FDA testing and allow each to claim their effectiveness in the treatment of hair loss. When you use Rogaine® and Prope-cia® together, as part of a Multi-Therapy treatment plan, these medications enable your hair transplant to gain greater hair density.
In February 2007 the FDA approved the HairMax La-
serComb, a medical device for the promotion of hair growth. 93% of the participants in the six month trial3 had an increase in the number of terminal (thick) hairs. Over 2500 research papers are published on lasers and no serious adverse events have been reported.
18 New Hair Restoration
Rogaine® Topical Solution (Minoxidil)
Rogaine was first administered internally to patients who were
suffering severe high blood pressure. As a side effect of the
drug, it was discovered that patients grew hair on various parts
of the body. Some patients who applied the 2% solution di-
rectly to thinning areas of the scalp found that the fine hairs
grew longer and thicker4.
Minoxidil is currently produced under the trade name
of Rogaine® Topical Solution and various other names. The medication's exact mechanism of action is unknown. It ap-pears to stimulate the hair follicles' active growth (anagen phase), causing the hairs to thicken and grow longer. Minoxi-dil is helpful in slowing down the rate of hair loss in approxi-mately 70% to 75% of patients, and about one in two patients actually experiences hair re-growth.
Rogaine® Topical Solution is available over-the-
counter (without a prescription) in both 2% and 5% concentra-tions. To be effective, the solution should be applied to the scalp once or twice daily. The recommendation is to shampoo and towel-dry your hair before applying the Rogaine® solu-tion. It is also suggested that you use a dropper applicator to spread the solution over the entire top of the scalp and allow it to absorb into the skin where it can do its work.
You need to understand that it will take at least two to
four months before you will notice less hair falling out, and six to seven months to see hair re-growth. Usually, this re-growth will be fine, short (vellus) hairs. Rogaine® must be used continually, as prescribed, over the long term in order to maintain its beneficial effects. If you stop using the medica-tion, the hair loss will recommence.
The main side effects of Rogaine®, which occur in ap-
proximately 2% of patients, are skin itching, scaling and
Methods of Halting Hair Loss 19
redness. Many of these cases can use a propylene glycol free
Minoxidil solution which may alleviate this.
Propecia® (Finasteride)
Propecia has been approved by the FDA as a remedy for hair
growth and for stopping hair loss.
Propecia significantly reduces DHT5, a key cause of
hair loss, by inhibiting the formation of DHT in your scalp.
Lowering DHT appears to inhibit the further shrinking of af-
fected hair follicles. DHT is a substance in the body that can
shrink the hair follicle until it no longer produces visible hair.
Propecia blocks the formation of DHT and, in this way, ap-
pears to interrupt the development of male pattern hair loss.
Propecia helps reduce further hair loss and re-grow visible
hair.
Propecia is made by MERCK & Co., Inc. Throughout
the world many hair restoration surgeons recommend it for their male patients who are distressed with hair loss. Hair sur-geons often prescribed Propecia after a hair transplant proce-dure.
DHT is shown in the following chart. Note that it
shows graphically what occurs when you simply let nature take hold of your hair growth, if you are genetically inclined to have thin hair or baldness.
20 New Hair Restoration
Reference MERCK & Co., Inc.
Methods of Halting Hair Loss 21
Alternative Treatments
Beware of Product Claims
As mentioned, be wary of products claiming to grow hair with
all natural ingredients and no side effects. Here are some cau-
tions about two popular ingredients:
There are several products on the market that contain
Minoxidil. Their manufacturers often disguise the identity of this ingredient by listing it under another name. While some of these products may yield results to some degree (because they contain Minoxidil), typically such products cost considerably more than Minoxidil in its generic form.
There are also many products that claim to contain Saw
Palmetto or other "natural" DHT blockers. DHT causes both hair loss and benign enlargement of the prostate gland, an organ in men that enlarges with age and can cause urinary problems. Clinical studies have shown that Saw Palmetto im-proves the urinary symptoms but does not act by lowering DHT. Nor does it lower prostate-specific antigen (PSA) or re-duce the size of the prostate. Most hair specialists do not rec-ommend the use of the various products containing Saw Pal-metto.
A hair system is a term for what is commonly known as
a wig or hairpiece. Hair systems are constructed from human or synthetic hair fibres and are attached to the head in a variety of ways, including:
• Glue bonding
• Weaving into your existing hair
• Various types of clips, taping or suction devices
Many hairpieces are left attached to the scalp for three to six weeks at a time before they are removed, cleaned and re-attached. The three most frequent complaints heard from pa-
22 New Hair Restoration
tients who have worn hairpieces say they are generally uncom-fortable, inconvenient and maintenance is expensive.
While hair systems remain a popular camouflage tech-
nique for hair loss sufferers, be sure to do your homework be-
fore you actually make a financial commitment to begin using
any system.
Low Level Laser Therapy
One of the latest innovations in medical technology is Low
Level Laser Therapy (LLLT). Low level lasers are referred to
as "cold" lasers because they do not release energy in the form
of heat. The light wavelength emitted from a low level laser
actually repairs tissues that have impaired cellular metabolism
by stimulating blood circulation and encouraging regeneration
of normal, healthy tissues.
During the 1960's and 1970's researchers used low level
lasers to evaluate their potential bio-stimulating effects on liv-ing tissues. In a surprise finding during experiments on pa-tients with leg ulcers, doctors observed that the hair follicles surrounding the area being treated by the low level laser grew new hair.
Laser light appears to stimulate micro-circulation, de-
crease inflammation and improve cellular metabolism and pro-tein synthesis. Furthermore, European studies suggest that LLLT increases blood and lymph circulation at the hair roots and stimulates follicular cells, which may cause hair to grow thicker and stronger.
Based on two modalities designed to treat hair restora-
tion patients, the Luce System LDS 100 System® and the new FDA approved HairMax LaserComb®, LLLT seems to have had a noticeably positive effect on the quality of hair growth with both surgical and non-surgical patients. LLLT can be used as a healing accelerator for post-operative surgical hair
Methods of Halting Hair Loss 23
restoration patients and many have found this therapy to aid
the healing process.
Multi-Therapy
Hair transplant surgery is an integral component of the Multi-
Therapy approach to hair restoration. It is the only permanent
solution for hair loss and is likely to remain so.
The following chapter examines the current surgical
technique called Follicular Unit Transplantation (FUT).
24 New Hair Restoration
Through hair restoration, this actor was able to achieve his
goal of more youthful roles in film and on stage.
Methods of Halting Hair Loss 25
This man wanted his hair line restored by filling in temples with
300 grafts on each side.
26 New Hair Restoration
This man received 1500 grafts to restore his front 1/3 hair loss.
Methods of Halting Hair Loss 27
This young man regained
his confidence after two procedures: 2100 grafts and 18 months
later 1500 grafts.
Best Hair Transplant Surgery 29
3 Best Hair Transplant Surgery
fter decades spent refining Follicular Unit Transplant
Asurgical techniques, hair restoration surgeons now have
the ability to transplant hair matching the way it naturally grows on the scalp. This is a significant achievement. While several earlier methods succeeded in permanently redistrib-uting hair from one part of the scalp to another, many of these transplants were not aesthetically pleasing. The older methods could not produce a natural-looking hairline.
How Hair Grows
Scalp hair - at the top, sides and back of the head - grows in
groupings of individual hairs. When viewed using 5-10 power
magnification, we can see clusters of one to four shafts of hair
growing from each follicle in the skin. We call these group-
ings "follicular units".
Typically, approximately 30% of scalp hair follicles
have one hair, 40% have two hairs and 30% of follicles have three to four hairs, but this varies from person to person.
There is an average of one follicular unit per one
square millimetre. As each follicular unit contains an average of 2 hairs, it is therefore possible to yield one thousand follicular unit grafts containing approximately two thousand hairs from a donor strip of scalp measuring one centimetre wide by ten centimetres long. With follicular unit grafting,
30 New Hair Restoration
doctors surgically harvest hair from the donor site keeping each unit intact.
Dissecting and Trimming Follicular Units
After the hair follicles are harvested from the donor site, the
resulting ‘donor strip' is maintained in a saline solution while
the surgical team dissects the individual units. This process is
explained in greater detail later.
As part of this process, it is essential to trim away the
excess epidermal and fatty tissue surrounding each follicle. This is a critical surgical step for two reasons. Firstly, each follicular unit must fit into the very small incision that forms the foundation of the new hairline. Secondly, trimming this tissue eliminates the occurrence of the unnatural pits and gaps between each grouping of transplanted hair.
These wide spaces contribute to the "pluggy" look in
patients who have undergone hair transplants performed by surgeons using older, less sophisticated surgical techniques.
Great precision is required for the dissecting and trim-
ming in order to preserve each precious follicle harvested for transplant and to prevent any damage that could compromise the viability of the newly transplanted hair. Powerful stereo-scopic operating microscopes enable surgeons and skilled technicians to clearly see each individual follicle within the unit being dissected, especially if the patient has very fine, blonde or white hair.
Best Hair Transplant Surgery 31
Transplanting Follicular Units into the New
Hairline
Following dissection and trimming, the follicular unit group-
ings of one, two, three or four hairs are individually and me-
ticulously implanted into each recipient site in the new hair-
line. As each tiny cluster of hair grows with very little skin
between the follicles, the patient will reap the benefit of a dra-
matically improved surgical hair restoration technique.
In a ‘mixed grafting' technique, single hairs are used in
the very front three or four irregular rows of the hair line.
Two-hair follicles are positioned immediately behind these
rows, followed by the three and four-hair follicles. The sur-
geon determines correct angulation, direction and orientation.
With this gradual increase in density coupled with an irregular
hairline, the surgeon can mimic nature, ensuring the outcome
is completely natural hence the surgical intervention is unde-
tectable.
How Many Follicular Unit Grafting Sessions
Are Needed?
For many patients, only two or three graft sessions may be
necessary to yield a completely satisfactory result. Indeed, one
transplant session is often sufficient for patients with limited
hair and modest restoration goals.
Follicular Unit Grafting and Mixed Grafting
Follicular unit grafting and mixed grafting hair transplantation
techniques offer patients superior hair restoration results. Pa-
tients no longer need to settle for the limited "thinning look."
Ideally, all patients want to achieve a result that is thick
and natural. In reality, patients' insufficient donor hair and/or financial resources usually restrict the surgeon's ability to ac-complish this "ultimate result". You may need to consider the
32 New Hair Restoration
trade-offs and then determine which surgical hair restoration option is best for you, considering your age, extent of your hair loss, remaining ‘donor' hair and your expectations.
Most patients elect to have the mixed grafting technique
performed. This enables them to enjoy the benefits of the most
natural looking hairline, composed of an irregular hairline and
variations in density and fuller, thicker hair (using the larger
grafts) for coverage behind it.
Former Hair Restoration Patients Often Seek to
Improve Upon Earlier Results
A highly skilled transplant surgeon can also treat men and
women who had surgical hair restoration procedures several
years ago. Recent transplant patients also seek to improve on
previous restoration results.
In many of these cases, while the patients' surgeries suc-
ceeded in achieving permanent hair growth on regions of the scalp that had experienced hair thinning and loss, they failed to look natural. Unfortunately, even though a surgeon may possess the technical knowledge to perform the new hair graft-ing techniques, he or she may lack the requisite design skills to create a truly natural-looking hairline. This all-too-common problem helps to highlight the need to do your homework be-fore choosing your surgeon.
Best Hair Transplant Surgery 33
Follicular and mixed grafting techniques offer an
undetectable, natural outcome for Alex.
34 New Hair Restoration
Bob had 2 procedures totalling 3,500 grafts – says "Nobody
knows I've had these transplants".
Best Hair Transplant Surgery 35
By the time he turned 32, he had lost most of his hair on top of
his head. The surgeon harvested the donor area, extracting 2000
grafts in two sessions that resulted in a much more pleasing
look.
36 New Hair Restoration
Robert is a computer programmer who wanted a permanent,
maintenance-free restoration. In two sessions of 3550 grafts, he
achieved his goal.
Greg, in his late 20s, wanted a more youthful appearance. He
felt that he was too young to have such bald areas on his scalp.
He got the results he wanted with two sessions of 3300 grafts.
Best Hair Transplant Surgery 37
Len regained his youthful
appearance after 3100
38 New Hair Restoration
Poor Results in the Past
Sadly, there are men and women who have spent years (and
large sums of money) in pursuit of their hair restoration goals
and have not succeeded. Hair loss is a dynamic process. While
the hair from follicles harvested from regions that are not sus-
ceptible to male pattern baldness and will grow permanently
where they are transplanted, it does not alter the fate of the
genetically predisposed hair around it. Unless these hair resto-
ration patients follow a course of medical therapy (Propecia®
Rogaine® and/or HairMax LaserComb®) as prescribed by
their doctor or hair restoration consultant, they will continue to
lose the surrounding non-transplanted hair.
In order to achieve your objective of a natural-looking
hair restoration with enough density to give you adequate cov-
erage, I strongly encourage you to find a skilled surgeon who
incorporates the Multi-Therapy approach to treat hair loss. A
consultation with your surgeon should ensure that your expec-
tations are in line with what is realistic and medically achiev-
able.
The Ideal Hair Restoration Solution for Many
In summary, more and more hair restoration surgeons are us-
ing follicular unit and follicular Micro Grafting techniques to
recreate and refine hairlines. By keeping the size of the hair
grafts as trimmed as possible and the units of hair intact, the
hair surgeon can create a truly natural-looking appearance.
These advanced surgical hair restoration methods are
well suited to treat both men and women who require limited hair grafting to achieve adequate scalp coverage. For the ma-jority of these surgical candidates, the new follicular unit grafting hair transplant methods present an ideal solution.
However, it is important to understand that there are still
limits to the degree of density that can be regained through
Best Hair Transplant Surgery 39
surgical hair transplantation, or any medical hair restoration treatment. While significant improvement in hair density can be realised through surgery (especially when patients follow a prescribed regimen of FDA approved medical therapies as well), the density will not equal the level a patient had prior to the onset of hair thinning.
The next chapter offers a review of important elements
of the surgical consultation.
For more information visit the website for the Interna-
tional Society of Hair Restoration Surgery – www.ishrs.com – and their articles on risk factors in hair restoration surgery and frequently asked questions: http://www.ishrs.org/surgical/surgical-complications.htm http://www.ishrs.org/mediacenter/media-faq.htm
40 New Hair Restoration
4 Hair Restoration Consultation
efore undergoing any medical or surgical procedure, it is
B always advisable to research your options and seek sev-
eral professional opinions. In this chapter, we will examine the
consultation phase of the hair restoration process. We also of-
fer valuable guidelines, which we hope you will use to take
control of your hair restoration from the very beginning.
Preparing for the Consultation
The primary objectives of this book are to inform you about
new medical and surgical hair restoration options and to em-
power you as a patient. It has been my experience that the
most satisfied hair restoration patients are those who invest the
necessary time and effort to prepare for the first consultation.
Visit the internet sites of reputable sources for infor-
mation about hair restoration. Once you have done this pre-liminary research, you may also use these resources to obtain the names of respected hair restoration surgeons in your area. Of course, an excellent means of finding a hair restoration surgeon is by personal referral. It helps to know a satisfied pa-tient or to ask your general practitioner or hairdresser for the name of a well-respected specialist.
42 New Hair Restoration
Consultations May Vary
Over the years, there have been compelling infomercials on
television about hair restoration. In the majority of these cases,
high-pressured sales tactics were commonly employed by
those advertisers in order to persuade prospective clients to
come in for a "consultation", where they met with a non-
medical (sales) representative who tries to sell a surgical pro-
cedure or hair system. This is classified as a "sales consulta-
tion", not a medical consultation.
Be cautious of anyone who tries to entice you with a
special discount or offer when you sign a contract and/or make a deposit that day—ESPECIALLY IF YOU HAVE NOT MET WITH THE DOCTOR OR TRAINED MEDICAL HAIR SPECIALIST. This is not how reputable hair restora-tion surgeons' practise. If you encounter this type of situation when you go in for a medical consultation, beware and seek the services of another doctor, even if you have to travel some distance.
Establishing the Doctor-Patient Relationship
The consultation is an opportunity for much more than a smile
and a handshake. It enables doctor and patient to get ac-
quainted on several levels. The initial meeting allows the doc-
tor to assess where a prospective patient is in terms of physical
hair loss, his area of greatest concern, what treatments may
have already been tried, how the hair loss impacts the individ-
ual on an emotional level, and more.
While talking with the hair restoration patient, the doc-
tor is also studying such characteristics as personality, facial features and aspects of the existing hairline—what features need to be accentuated and what should be minimised. At this stage, the doctor is already planning how he or she will place different groupings of hairs in different patterns to best suit
Hair Restoration Consultation 43
that individual. Taking time for these details enhances the doc-tor's ability to formulate a superior treatment plan and hairline design for the patient.
From a patient's perspective, the consultation is your
time to learn as much as you can about the doctor, the practice and your hair restoration.
Now is the Time to Determine Objectives and Dis-
cuss Expectations
The consultation serves both patient and doctor as you work
together to determine your hair restoration objectives, review
various medical and surgical solutions, and obtain a clear un-
derstanding of what you can realistically expect as a final re-
sult.
During your initial visit, you need to know the doctor's
professional assessment of your condition, including an accu-rate determination of where you are according to the Norwood or Ludwig scales of male/female pattern baldness; what you can realistically gain in terms of density; the doctor's detailed treatment plan and fee for services.
This discussion must also set appropriate expectations
in terms of the actual numbers of sessions and grafts required to achieve your hair restoration objectives. You may discover that you need more sessions than you had anticipated. For ex-ample, the fact that you have dark, straight hair and light skin may require more work. Or your donor area may be insuffi-cient and this will limit the doctor's ability to achieve the de-sired density.
Additional Considerations
Here is a partial list of questions to ask your doctor:
• Please tell me about your medical training and back-
44 New Hair Restoration
• How did you get interested in the field of hair restora-
• How long have you been performing hair restoration
• How many surgical procedures do you perform in a
day? Many factors determine how many surgeries a doctor can perform. One or two is reasonable.
• Do you offer a Multi-Therapy approach to your pa-
• Do you use Follicular Unit Grafting, Micro Grafting
and Mixed Grafting surgical techniques?
• How much of your practice is dedicated to medical
and surgical hair restoration?
• What will your role be in my surgery? Will you actu-
ally make all of the incisions and place each graft? In many clinics, the doctor only removes the strip and is NOT involved in the important design, or in the graft placement.
• What training and experience does each member of
your medical and surgical team possess?
• How often do you and your staff go for continuing
education related to medical and surgical hair restora-tion?
• Are you an active member of any professional hair
restoration organizations? Which ones?
• Please give me the names and contact information of
patients I can call as referees.
• Please show me your patients' Before and After pho-
Guidelines for Evaluating Before and After
Photographs
• For each photo, ask the name of the surgeon who per-
formed the surgical procedure on the patient.
• Can you see the patient's hairline in each photo?
Hair Restoration Consultation 45
The most detectable part of a hair transplant is the 2-3 cms. You need to see the hairline in order to deter-mine if the doctor used follicular unit grafts.
• Study the hairlines.
• Do the hairlines curve around near the temples?
• Are hairlines straight across or staggered?
• Do the hairlines appear natural and random?
• Ask yourself, "Does the patient's hairline look right?"
You do not need to be an expert. You can certainly judge whether or not a hairline looks natural.
• Clinical Before and After photos should not be re-
• Not all hairlines should be created equal. You need to
see that the doctor can produce a variety of hairlines that are appropriate to the age, hair characteristics and facial structure of each individual.
• Watch for the "high and wide" hairline.
• Be sure you see photos taken from different angles.
The photos provided should enable you to evaluate coverage, density and appearance from multiple an-gles.
• Ask for an overview of each patient's treatment plan.
• What was the surgical treatment plan?
• How many grafts did the patient receive?
• What size grafts?
• Had the patient had any previous hair restoration sur-
gery? If so, how many procedures?
• Was any adjunctive therapy used? (e.g. medical, la-
ser/phototherapy, nutritional supplements)
• Was the patient on Propecia?
• Did the patient use Minoxidil?
• How many months after the procedure were the pho-
• Which doctor performed the surgery shown in each
photo? Unless the question is asked, it may not be disclosed that different doctors performed surgeries
46 New Hair Restoration
on different patients showcased in the practice's port-folio. In fact, an individual patient may have had mul-tiple procedures which may have been performed by different doctors.
Many practitioners bring their unique medical back-
ground, philosophy and preferred approach to their work and hair restoration practice. The consultation and medical evalua-tion process varies between doctors.
In the next chapter, there will be an elaboration on the
medical evaluation, which may be conducted at the same visit as the consultation and also review common pre-operative protocols and considerations.
Hair Restoration Consultation 47
Excellent hair characteristics achieved a re-
markable result with 3,000 follicular units.
48 New Hair Restoration
5 The Medical Evaluation
air transplantation is a cosmetic surgical procedure. Al-
Hthough it is considered minor surgery and typically per-
formed under local anaesthetic in an outpatient facility, every
patient must undergo a thorough medical evaluation before
surgery can take place.
The Medical Evaluation Is Not the Same
As a Consultation
The consultation is an essential part of a patient's information
gathering and decision-making process. Generally, once the
patient has chosen a doctor and hair restoration solution, the
medical evaluation follows as the next step. During the pa-
tient's medical evaluation, the doctor must gather relevant pa-
tient information in order to make critical decisions for the
patient's course of treatment and medical care.
Remember, whether you are still in the decision-
making stage or you are actually in the midst of a surgical
procedure, it is always appropriate to ask questions. If you do
not understand an answer, be sure to say so. Clear communi-
cation between doctor, patient and the entire medical team is
vital to ensure a safe, satisfying and successful outcome.
50 New Hair Restoration
Completing the Medical Questionnaire
In most cases, you will be asked to complete a written medical
questionnaire prior to your medical evaluation. In many of-
fices, doctors request this information at the initial consulta-
tion.
Not only is it in your best interest, it is critical that you
answer each question as accurately and completely as possi-ble. Your doctor will rely on your answers in order to make decisions that will affect your hair restoration. Your doctor must be aware of any specific underlying medical conditions, diseases and issues you may have—past and present.
Requesting Medical Clearance
Prior to undergoing a surgical procedure, the hair restoration
surgeon may require medical clearance from your general
practitioner.
A hair restoration surgeon will request your general
practitioner's clearance for surgery to ensure your medical his-tory, physical examination findings and appropriate diagnostic test and lab results indicate that it is medically safe to proceed. Your general practitioner may require that you submit to an electrocardiogram (ECG).
The results of recent laboratory blood tests may be
necessary. These include FBC with platelet count, prothrom-bin time, Hepatitis and HIV testing. If you have undergone this blood-work within the past year, your doctor may allow the lab to send a copy of your results to the office without re-quiring new tests to be performed.
Upon reviewing patient consent, the hair restoration
surgeon may ask that your general practitioner disclose any prescribed medications as well as the doctor's medical opinion regarding the status of your medical conditions, including al-lergies, cardiovascular disease, hypertension, blood-clotting,
The Medical Evaluation 51
infectious disease status, substance abuse and psychiatric dis-orders.
It is important to remember that there are certain medi-
cal conditions and issues which may prohibit a patient from undergoing surgical hair restoration or taking medications such as Propecia®.
Medical Evaluation by the Hair Restoration
Surgeon
The medical questionnaire and evaluation give both doctor
and patient the opportunity to discuss allergies, medication,
special considerations and accommodations needing to be ad-
dressed.
In addition to questions and answers related to a pa-
tient's medical history, I evaluate each patient's hair loss his-tory.
Hair Loss History
The hair surgeon needs to know as much as possible about
each patient's hair loss in order to determine the best hair res-
toration solution and treatment plan appropriate for the indi-
vidual.
• When did you begin to lose your hair?
• Has your hair loss been gradual or sudden?
• What is your family history of hair loss? (Who suf-
fered from hair loss: mother, father, maternal grandparents, paternal grandparents, brothers, sis-ters, cousins?).
• How are you coping with your hair loss? How does
your hair loss affect you on a daily basis?
• How have you addressed your hair loss? (Have you
tried medication such as Propecia® or Rogaine®,
52 New Hair Restoration
supplements, special shampoos or lotions, camou-flaging products?)
• Have you worn a toupee, wig or hair system?
• What has not worked for you and why?
• Have you ever undergone a surgical hair restora-
• Do you lead an active lifestyle (e.g. Do you swim,
play tennis, work out, etc.)?
• What are your hair restoration objectives? Do you
want to achieve minimum or maximum coverage? What about a permanent solution? Is there a way to stop hair from falling out? Do you want to grow more hair? Can an unnatural-looking transplant be improved?
• Where are your priorities regarding coverage?
Front hairline, mid-scalp, crown, entire head?
While these are basic questions, it is a mistake to as-
sume your doctor will know what you consider to be impor-tant. You have to tell the doctor what you want! You need to clearly communicate with your doctor and the medical hair restoration team.
The Hair and Scalp Examination
Hair and scalp examinations vary with each doctor. For the
purposes of this book, I will explain the more common ele-
ments of this part of the medical evaluation.
Hair restoration surgeons must evaluate the patient's
hair colour, texture and type in order to develop the surgical plan. Examination of the hair follicles and hair density under magnification allows more accurate assessment of the number of grafts and sessions required to achieve the restoration ob-jectives.
The Medical Evaluation 53
In cases where there has been previous surgery, the
donor area will need to be examined to determine how many grafts may be extracted from the remaining tissue and the ex-tent and condition of the scarring.
Previous transplant work should be closely examined
to determine the ideal approach to achieve the best surgical outcome.
Hair and scalp examination to determine the qualities
of the donor hair.
54 New Hair Restoration
6 Follicular Unit Extraction
ollicular Unit Extraction (FUE)—also referred to as the
F "FOX" technique—enables surgeons to minimise scarring
in the donor area of people who have very thin hair. For some people, the idea of having a linear scar, however narrow, is unacceptable. This surgical technique provides another option for harvesting or "extracting" from the scalp to provide donor hair.
With Follicular Unit Extraction, surgeons are able to
extract single follicular units (groupings of 1, 2 or 3 hairs) in-dividually from the donor area without a scalpel. Follicular Unit Extraction is a less invasive procedure than the strip har-vesting method normally used in surgical hair transplantation and also means the patient will not require stitches.
At the moment there are few doctors performing Fol-
licular Unit Extraction worldwide. While some hair restoration surgeons are doing 14-hour procedures and harvesting 1500 grafts using the FUE method, the same result can also be achieved over multiple sessions. The surgeon and staff may perform a second procedure within days of the patient's first FUE session. In some cases, the doctor may do the right side of the donor area on one day and the left or centre area the fol-lowing day.
56 New Hair Restoration
Advantages and Disadvantages
There are several post-operative benefits associated with Fol-
licular Unit Extraction. Patients walk out of the procedure
with the follicular units implanted as they would with a tradi-
tional procedure, but there are no stitches in the donor areas
and therefore less discomfort. The tiny circular incisions be-
come nearly invisible within a matter of days.
While the benefits of Follicular Unit Extraction are
quite appealing to many prospective hair restoration patients, it is a tedious process for the surgeon and the surgical team because it requires much more time to harvest the same num-bers of grafts compared with the strip method. Currently, most qualified surgeons are able to harvest between 500 – 700 grafts within a five to six hour period using the FUE method. As the individual grafts are harvested ‘blind' the likelihood of graft transection is high. Studies6 suggest that graft mortality could be as high as 35%, as well as many multi-hair follicles being harvested as single hairs. This means that the total hair yield could be as little as 20% of what is possible using strip grafting!
This procedure is also still cost prohibitive for many
patients. The time and cost required for a Follicular Unit Ex-traction procedure that yields 500 – 600 grafts is approxi-mately the same as that currently required to yield 1700 – 2000 grafts using the strip method.
Follicular Unit Extraction 57
Stay Focused on Finding the Right Surgeon
It is very important for patients to understand the importance
of choosing the right surgeon for a satisfactory outcome. Final
hairline design results are dependent on the skill and artistic
abilities of the surgeon performing the procedure. People often
make the mistake of concentrating too much on how the doc-
tor will extract the grafts and forget the basic rules that apply
to artistic hairline design. Therefore it is critical that prospec-
tive patients evaluate a surgeon's proven expertise using the
Follicular Unit Extraction technique in addition to the doctor's
demonstrated artistry recreating undetectable, natural-looking
hairlines.
Are You a Candidate for Follicular Unit
Extraction?
Here are a few questions for you to consider: • How many grafts will be needed to get the job done?
(If you need too many grafts, the procedure may be time and cost prohibitive).
• How long is the hair on the back of your scalp? • Why waste your time and money on this procedure if
your hair will easily cover a scar the donor area?
• Are you on treatments to stop the progression of your
hair loss? If you are not, and your hair loss continues, you will need to continually fill in the areas where you are losing hair.
If you are considering a hair transplant or a Follicular Unit
Extraction procedure, you should discuss the options and their suitability for you with a hair restoration surgeon or consult-ant.
58 New Hair Restoration
For more information visit the website for the International
Society of Hair Restoration Surgery - www.ishrs.com - and their article on follicular unit extraction: http://www.ishrs.org/articles/hair-follicular-units.htm
Enhanced hairline.
Enhanced hairline.
Enhanced hairline.
7 Preparing for Surgery
nce you and your doctor have determined that you are a
O candidate for surgical hair restoration, it is normal to look
forward to the day of surgery with both anticipation and some apprehension.
The best way to overcome anxiety is to be prepared. Take
time to learn about each of the various hair restoration options available to you. Be sure to call and meet with some of the pa-tients who have undergone surgical procedures with the doctor you are considering to perform your hair restoration surgery.
By learning about hair restoration, you will be more con-
fident as you prepare for surgery.
Listening to Your Doctor and Following
Instructions is in Your Best Interest
Usually during or immediately following the medical evaluation
the surgeon or consultant will review all of the necessary pre-
operation instructions with the patient. On the following pages
are some of the common guidelines used by doctors to acquaint
you with important considerations regarding hair restoration sur-
gery.
The importance of listening to your doctor's instruc-
tions and following the pre and post-operation guidelines you
will be given cannot be emphasized strongly enough.
60 New Hair Restoration
The following section is not intended to replace the medi-
cal advice or instructions given by your surgeon or hair trans-plant consultant. It is not an exhaustive list, but it will serve as a review of the general guidelines patients need to follow prior to undergoing hair restoration surgery.
Complete and Send Results of Required Lab Work
to Your Doctor
Prior to surgery, as we mentioned earlier, lab work may need to
be completed. Some surgeons offer lab services on the premises
of their facilities. Others will ask the patient to visit their GP or
refer patients to reputable medical laboratories nearby.
It is important to provide any medical information and test
results required by the surgeon to enable him or her to make im-portant medical decisions and to ensure the quality and safety of your medical care.
In the Month Prior to Surgery
It is suggested that patients allow hair to grow around the donor
area, at the back of the head from where hair for transplant will
be harvested, for approximately four weeks if possible. Longer
hair will help to conceal the surgical incision required to harvest
the donor strip of scalp.
In the Two Weeks Prior to Surgery
It is essential to avoid being sun burnt in the two weeks prior to
surgery. Your surgeon will also advise you to avoid vigorous ex-
ercise, including running or lifting weights, for the week preced-
ing surgery. Such activity can lead to increased bleeding during
surgery.
If you use a laser comb, you may be advised to cease us-
ing it before the surgery and for a short time afterwards.
Preparing for Surgery 61
Medications and Supplements
It is important to inform your hair restoration surgeon about
every vitamin, nutritional supplement, over-the-counter medica-tion and prescription drug you currently take. Your doctor must also know if you are using any illicit or recreational drugs, e.g. marijuana, cocaine, "club drugs," and so forth. This is vital in-formation to share with your doctor because he or she must be prepared to address potential drug interactions and make critical decisions relating to your surgery to ensure your safety, comfort and healing.
Your surgeon will instruct you to stop taking substances
that thin the blood in the three days prior to surgery. Some of the common items to avoid include aspirin and products containing aspirin, non-steroidal anti-inflammatory drugs such as Ibupro-fen® and Naproxyn®, Vitamin E and multiple vitamins which contain Vitamin E, Ginseng, Ginko Biloba and Garlic pills. Ty-lenol and other Paracetamol-based drugs are usually permitted.
If you are on any prescribed medications you must inform
the surgeon of these and confirm whether the drugs should be continued or temporarily stopped prior to the surgery.
Alcohol and Nicotine
Alcohol or nicotine may cause unnecessary problems during and
after the operation.
While it is always advisable to limit alcohol consumption,
you will be asked not to drink alcoholic beverages for 48 hours prior to surgery.
Smokers and non-smokers must avoid or minimise nico-
tine and second-hand smoke for 48 hours prior to surgery. Nico-tine is found in tobacco products including cigarettes, cigars, pipe and chewing tobacco, Nicorette® gum and prescription patches.
Poor growth post operatively has been reported in
heavy smokers and those with severe sun damage.
62 New Hair Restoration
Minoxidil and Hair Products
If you are using Rogaine® (Minoxidil) some surgeons advise
patients to discontinue its use three days prior to surgery. It is not
necessary to stop the use of Propecia®.
Hair colour and/or permanent wave (perm) processes
must be done no later than two days before surgery. Some doc-
tors recommend this be done one to two weeks prior to surgery.
Patients may begin colouring/perming their hair again two weeks
after their surgical procedure.
Procedure Confirmation
It should be standard procedure for your surgeon's office to call
and confirm your surgical appointment. If not, be sure to confirm
your surgery a few days before your scheduled procedure.
Transport
Because a mild sedative and local anesthetic are used during sur-
gery, you will not be able to drive yourself home following your
surgical procedure, or for 48 hours afterwards. It is therefore
necessary to arrange transport to and from the clinic. The clinic
will be able to call you a taxi if you do not have a private lift.
Patients living more than a 90-minute drive from the sur-
gical facility should arrange for overnight accommodations near-by. In most cases, the clinic office will be happy to provide rec-ommendations for hotels in the vicinity.
The Day of Surgery
On the evening before or on the morning of your hair transplant
procedure, shampoo and condition your hair. Do not use any oth-
er hair products such as hairspray, mousse or hair gel.
Wear a shirt that unbuttons completely down the front.
Do not wear any garment with a close-fitting neck that would be difficult to put on or remove over your head. Wear comfortable clothes, as you will be seated for several hours. Bring a clean hat
Preparing for Surgery 63
such as a baseball cap with you that you can wear afterwards. A close-fitting hat such a beanie is not suitable.
Before arriving at your surgeon's clinic, eat a light meal
and take prescribed medications as normal. It is important to have an adequate blood sugar level and enough food in your stomach to absorb your medication. You may also be given a light snack during the procedure to maintain your blood sugar levels.
This advice may seem contrary to what has been directed
before by other surgeries. This is because hair transplantation is minor surgery, so only a local anesthetic is administered. Patients are required to fast only before undergoing surgeries that require general anesthesia.
You may also be asked to avoid coffee, tea and any other
beverages or foods containing caffeine. Caffeine, like nicotine, is a stimulant.
Finally, arrive promptly at the requested time to settle any
outstanding payment and sign the surgery consent form. Most surgical hair restoration practices require an initial deposit and payment of the balance to be paid on the day of surgery.
Be Comfortable and Prepared
Following the suggested guidelines outlined throughout this
chapter will give you added peace of mind and ensure a safer and
more comfortable surgery.
Most patients feel confident with their decision to un-
dergo this procedure when they have a better understanding of what to expect.
In Chapter 8, we will describe the micro-follicular unit
transplant method of surgical hair restoration in detail.
64 New Hair Restoration
Patient prior to surgery, with hairline and extent of recipient
area marked with washable pen.
Preparing for Surgery 65
Planning the Transplant to suit individual patient.
66 New Hair Restoration
8
Hair Restoration
Procedure
Hair transplant procedure is permanent.
Once the new hair grows there is no need for special care or
maintenance; the transplanted hair will continue to grow natu-
rally. Under normal conditions the transplanted hair will grow
and appear as normal with the rest of the hair. Since hair
transplantation is the harvesting of healthy donor hair from the
body (back of head, side of head, chest, back) and implanted
in the scalp, or in other areas where you may wish to have hair
growth, it will grow and fill in bald areas.
Anaesthesia and Medication
When you arrive at the clinic, you will be given a gown and
medication before we begin the transplant procedure. Be sure
to use the bathroom before the procedure.
I will reconfirm the surgical plan and mark the area for
treatment directly on your scalp in consultation with you. I offer intravenous sedation, antibiotics and medication to re-duce pain and swelling. In preparation of donor and recipient sites on your scalp, a staff member applies antiseptic to the site. Sedation is then given. The area is numbed with injec-tions of anaesthetic, which you do not feel as you are sleeping.
68 New Hair Restoration
Patient in theatre immediately before surgery. Markings
in green pen show the extent of recipient area.
After an injection of local anaesthetic there is generally
no discomfort during the entire procedure. You will drift in
and out of sleep during the procedure. Should there be any
minor discomfort the surgeon will administer additional medi-
cation. All you need to do is relax and dream about all that
new hair!
The Donor Strip to be Harvested
Before the donor strip is removed, the area is measured and
the hair in the designated region clipped short, local anaes-
thetic numbs the area before the donor strip is removed.
The wound is usually closed using a trichophytic
method that is, one edge of the wound is trimmed away with the other edge overlapping to allow the hairs near the edge of the wound to grow through the scar. The benefit is that it pro-duces undetectable scars in most patients.
Hair Restoration Procedure 69
A double layer closure with two types of suture mate-
rial creates the best approximation of the wound edges and causes less pain in the healing phase. The non-dissolving su-tures are removed after 10 to 14 days while the dissolvable sutures absorb over 3 to 4 weeks.
Many individual factors can influence healing and the
long term appearance of surgical scars. People with connective tissue diseases, keloid production, hypertrophic scarring and naturally tight scalps are more prone to scarring.
Post operative care is important. Minimizing strenuous
activities and limiting movement of the head and neck for the first few weeks will allow for more effective healing.
The scalp tissue is maintained in chilled saline solution
while grafts are being prepared by a team of highly trained technicians. The hairs are cut very carefully into their natural grouping of one to four hair follicles to ensure optimum growth and survival of the grafts. The preparation and place-ment of the grafts is extremely labour intensive with a proce-dure of 1500 grafts taking a team of 5 to 6 people up to 4 or 5 hours. It is essential to have a dedicated highly skilled team of technicians assisting in the surgery.
70 New Hair Restoration
The upper photo shows a normal closure while the lower photo
demonstrates the ‘invisible' scar achievable with trichophytic
closure. These photos are of the same procedure on the same
patient where each half of the donor closure was treated by the
two different methods.
Hair Restoration Procedure 71
Follicular Units
As you can see in the photo here hair follicles or follicular
units tend to cluster in two or more units; these are seen as
natural clusters of hair follicles. During the process of harvest-
ing, the follicular units are dissected in a sterile, small lab by
highly trained technicians with a high survival rate when
placed on a tray ready to be placed in the scalp or other site.
Most follicular unit Micro Grafts measure 1/2mm to 1 mm
across, smaller than a grain of rice.
This shows naturally occurring follicular clusters of 1, 2, 3, and
4 hairs. It is from clusters such as these that follicles are re-
moved and placed where needed for new growth.
Hours may pass between the time donor grafts are re-
moved from the back of the head to the time they are im-planted in the scalp. The donor tissue and individual grafts are kept moist at a cool 4-5°C until they are implanted in the scalp.
72 New Hair Restoration
Note how each section of the strip is removed and dissected
into 1, 2, and 3 follicular units.
The purpose of using single follicular units is to obtain a
natural look. For the hairline, I use single follicular units. These single units are the best options for the hairline. For density purposes, I prefer to use the larger follicular units for the coverage of the rest of the area. The goal in a hair trans-plant is the combined result of an undetectable hairline and added density for the other areas of the scalp.
Hair Restoration Procedure 73
Follicular units.
Use of single follicular units and a "Snail Track" hairline
resulted in this natural looking hairline.
74 New Hair Restoration
Recipient Site
After the harvesting of the follicular units and during the dis-
section of hair follicles, I review the markings to be certain
that they are drawn to allow for the best natural appearance,
meaning, that the new grafts will grow out in the most natural
way possible. This has to do with the angle of placing the
grafts to achieve a similar pattern where hair once grew. The
angle at which the grafts are placed is crucial to achieve a
similar pattern to where hair once grew. It is critically impor-
tant that careful attention is paid to graft placement to ensure
that no damage takes place to existing hair follicles and cor-
rect spacing between each graft is achieved.
Whilst the individual grafts that have been dissected un-
der the microscope are completed, I make incisions in the scalp to accept the Micro Grafts. The slits made as the recipi-ent sites will determine the pattern and direction of hair growth. This is a critical step. I will make small slits in the marked scalp with a slender flat-bladed surgical instrument developed specifically for this purpose. The small slits allow grafts to be placed between growing hairs and transplanted hairs. They do this with less risk of damage to the adjacent hairs, thereby increasing hair density.
Both the length and the depth of the slits are important
for the hair transplant. The microcirculation is just beneath the hair follicle; if the incision is too deep this can compromise hair growth. It is essential to minimise trauma to the surround-ing tissue by tumescing or puffing out the recipient area with saline.
The older graft technique required greater spacing be-
tween the grafts for proper blood flow in order for the larger grafts to grow properly. This created a less dense appearance and often resulted in a tufted (toothbrush like) impression.
Hair Restoration Procedure 75
Dense Packing
This is a skill of placing the follicular units close together to
ensure a natural result in a single pass. For example, the
transplanting of a hair line requires dense packing in order to
achieve a natural look with no gaps should be evident. The
amount of follicular units to be placed may vary depending
on certain factors such as hair shaft quality, ethnic origin,
hair characteristics, hair colour, curls and existing hair den-
sity.
Mega-sessions
A Mega-session can only be performed when a patient
has a high density donor hair available for strip harvesting at the back or sides of the head. The patient has to have appro-priate skin laxity.
We consider a mega-session to be more than 1,500 grafts
implanted in the scalp in a single session. A super mega-session involves more than 2,500 grafts. These mega-sessions will take six or more hours to perform and require a team of highly trained technicians to work efficiently at a rapid speed ensuring quality control of all follicular units required for im-mediate implantation. At all times the patients interest must come first which includes the minimization of trauma. Hence, speed and accuracy is paramount, to achieve an optimum out-come.
The technicians supporting the mega-sessions consist of
a placer, sliverer and an expert cutter, often more than one of each.
76 New Hair Restoration
Patient immediately after transplantation of 2200 grafts.
Same patient two days later.
Hair Restoration Procedure 77
Placing Individual Grafts
The graft placement phase of the procedure could require
more than two hours. The amount of grafts required is pre-
determined by the patient and the surgeon prior to procedure.
In the various parts of the scalp, hair grows at different
angles. This is a part of your pre-determined hair characteris-tics. My task is to mimic nature. I place the transplanted hair in the appropriate position, correct angle, direction and orien-tation to give a natural undetectable and pleasing appearance. Replicating your own individual hair characteristics is the hallmark of an excellent hair transplant. Other attributes I have to pay attention to are the spacing of each individual follicle, the depth of the incision and your unique hair pattern. Your transplanted hair will need to fall in line with your neighbour-ing hairs to establish a natural flow, symmetry and appear-ance.
In nature, in order to optimise coverage, the hair's direc-
tion is always coronal. The incisions for the hairs are made at right angles to the direction of growth. If this pattern of hair transplant is followed your hair will flow in a natural, easy-to-manage fashion. This is where the surgeon's observation skills, artistic flair and technical competence come to the fore.
78 New Hair Restoration
The angles at which the hairs grow vary on different parts of
the scalp. The correct angle of the incision for the recipient site
is essential to achieve proper flow.
To achieve a satisfactory and pleasing result the surgeon
will work through any existing hair. There is usually no need to trim the existing hair, which will cover the short trans-planted follicles.
Hair Restoration Procedure 79
Optimum Density
There are several factors to consider in order to achieve an op-
timum long term outcome. Since hair loss is continuous
throughout life, hair suitable for transplanting is a limited re-
source and individual's expectations vary as they age; the sur-
geon has to include all of these unknowns to anticipate the pa-
tient's long term needs. The patient's present expectation of
density will change over the years. Optimum density is influ-
enced by the existing extent of hair loss, future hair loss, col-
our, hair characteristics, contrast between skin and hair, along
with the number of future sessions that may be required to
achieve the optimum benefits of grafting.
The chart below indicates an approximate total Number of
Follicular Unit Grafts required to make a complete restora-
tion (subject to patient's hair characteristics)
80 New Hair Restoration
Eyebrow transplant to camouflage previous scars.
Sideburn reconstruction after facelift to hide scars.
Face and Body Hair Placement
Hair can be transplanted to almost anywhere on the face and
body. Most often it is the balding scalp where patients seek
follicular hair restoration, but there are those who may have a
need for eyelashes, eyebrows, sideburns, whiskers, pubic re-
gions and other locations of the body. The follicular units will
grow in any of these locations. Injury to the body due to an
Hair Restoration Procedure 81
accident such as burns, cuts and skin damage are special cases where a restoration of hair may be needed. These special areas require skills on the part of the surgeon and the aim is to achieve the best possible results wherever there is need for hair replacement.
Most often hair is harvested from the scalp in the do-
nor region. It will typically grow as normal hair would on the
head. The hair taken from the scalp usually requires monthly
trimming to maintain a natural appearance.
Scar before and one year after one session of grafts.
Scars
It is possible to remedy the effects of scarring on the scalp.
There are various types of scars; atrophic, thick (hypertrophic)
or keloid (genetically thickened scars). A mature scar com-
prises dense, non stretch collagen bundles which allow only
poor hair growth. To encourage good hair growth of hair
when transplanted, I have developed a technique that allows
for a more predictable growth.
82 New Hair Restoration
Brow lift scar and one year after one session of grafts.
Hair Restoration Procedure 83
Burns treated with one session.
One year after revision.
84 New Hair Restoration
Immediately following Surgery
Following the procedure when the sutures are in place, a staff
member will clean the donor area and inspect the results, at
this point you would be encouraged to ask questions. Healing
time begins at that point and could take up to 7 days depend-
ing on the individual. Before you depart the surgery the su-
tured area will be wrapped with a sterile bandage. The follow-
ing day the bandages will be removed by the patient and a
visit to the clinic is not required. Most patients do not need
bandages on the recipient site. Photos are taken and the pa-
tient may go home on advice of the surgeon and staff.
After Surgery Appearance
Follicular unit procedures typically result in a slightly unnatu-
ral look immediately following the surgery.
Crusts form from dried blood and individual patients
heal at different rates. The crusts may last for a few days after the procedure and it is important not to allow the recipient area to get wet during this time. After three days the scalp can be gently washed and the grafts will become practically unno-ticeable. Patients often wear a hat or a cap during this time. Usually patients choose to take a few days off work, until the grafts are no longer evident.
Hair Restoration Procedure 85
Patient 7 days after surgery with a few scabs in hair
86 New Hair Restoration
The same patient after 3 and 6 months.
Hair Restoration Procedure 87
Permanent Loss
Transplanting hair includes a risk of permanent loss of some
or all of the transplanted donor follicles. Typically the yield of
transplanted grafts is greater than 90% and often approaches
100%. Lower yields can occur, especially if a scalp infection
occurs and is not properly treated, or in "massive mega-
sessions" involving thousands of grafts in a single session,
blood supply is compromised.
About two weeks after surgery the transplanted hair will
fall out. This is normal. The follicles, transplanted into the
scalp, remain. The follicles will grow a new hair in the follow-
ing few months.
With the application of Propecia™ and Follicular Unit
Transplant, this 38-year-old male achieved acceptable results.
88 New Hair Restoration
Dennis, a 55- year- old pa-
tient wanted to transit from
wig to hair. He had an ex-
cellent donor area. After 2
sessions of 2500 and 900
graft transplant, natural
hair appearance was
achieved.
Hair Restoration Procedure 89
Forty-five year-old man with a wonderful head of hair
compared with months earlier. He had an abundance of
hair on the back of his head that was harvested and trans-
planted to the sparsely covered frontal part of his head.
90 New Hair Restoration
John had 1500 grafts to
enhance hairline and
mid scalp.
9 Women's Hair Loss
air loss in women is less common than in men but can
Hhave a far greater effect on self esteem and confidence.
Female hair loss is also more widespread than realised, be-cause women will go to great lengths to disguise any bald patches or general thinning.
Hair loss in women can be due to genetic factors. This
is called androgenic alopecia (or female pattern hair loss – FPHL), and can be noticed at any age from puberty to 40 years of age. Up to 50% of women will be affected by hair loss due to genetic factors in their lifetime.
However hair loss in women can also be caused by a
variety of other factors including hormonal imbalances or changes, dietary deficiencies, stress, illnesses or some medica-tions such as anti-cancer drugs, hair styling and chemical hair treatments. It can also be triggered by events in a woman's life, such as menopause, child birth, a trauma or major opera-tion.
Any women affected by hair loss, whether short or
long term, diffuse thinning or bald patches, should be assured that they are not alone, and treatment is often possible. De-pending on the cause, a hair restoration specialist can recom-mend treatments to reverse the hair loss, and relieve some of
92 New Hair Restoration
the associated social anxiety. Hair loss is a medical condition,
and a woman suffering hair loss should seek a medical opinion
and medical treatment. If left untreated, hair loss can progress.
Psychological Effects and Coping with
Hair Loss
The psychological effects of hair loss in women should never
be underestimated or disregarded. Due to social and cultural
expectations, hair loss can be more distressing for a woman
than for a man. Bountiful hair is seen as integral to a woman's
sexual attractiveness and femininity. While hair loss is gener-
ally regarded as normal in men, women are more likely to be
concerned and anxious about the ageing effect of thinning
hair.
There are various different causes of hair loss in
women. The correct diagnosis is required before a suitable
treatment can be recommended. Dr Marty Sawaya, a derma-
tologist and specialist in hair loss, explains "The emotional
impact for women with thinning hair is tremendous. One of
the major roles of the doctor is to help women understand the
various reasons7 for hair loss, helping them to focus on realis-
tic treatment options and expectations to optimise treatment
outcomes."
Stages of Pattern Hair Loss in Women
Recent evidence suggests that female pattern hair loss is a dif-
ferent inherited disease from pattern hair loss seen in men.
Female pattern hair loss shows a complex inheritance, so the
distribution and degree of hair loss among women in a family
is not as predictable as that in men.
In women there is often generalised diffuse thinning
over the entire scalp. Hair loss can also be localised, leading to
Women's Hair Loss 93
a mosaic of patchy loss, or loss along the central parting on the top of the head.
Ludwig developed a classification system for pattern
hair loss in women, in which Stage I is described as thinning hair on the central scalp, Stage II is thinning hair and greater patches of scalp hair loss and Stage III shows male-pattern hair loss at the front scalp to mid-scalp. It is extremely rare to see advanced hair loss in women.
It can also be triggered by events in a woman's life,
such as menopause, child birth, a trauma or major operation.
With Stage II hair loss, this woman initially wore a wig. The wig
being uncomfortable, she decided on a permanent solution. Af-
ter a hair transplant of 2500 grafts, she is pleased with the re-
sults of this decision.
What Causes Hair Loss in Women?
Hereditary pattern hair loss, or androgenic alopecia, is less
common in women than in men. Early diagnosis of female
pattern hair loss can be difficult because hair loss in women
can be caused by many other factors, such as illness or hor-
monal changes. For this reason, a doctor or hair restoration
specialist will ask for medical history, any possible contribut-
ing factors including pregnancies or onset of menopause and
order a set of blood tests.
94 New Hair Restoration
Irregular hairline rectified by a small transplant.
The blood tests will include a full blood count (FBC),
iron (Se Ferritin), thyroid stimulating hormone (TSH), blood sugar level (BSL), follicle stimulating hormone (FSH), estra-diol (E2) and erythrocyte sedimentation rate (ESR), a non-specific screening for various diseases. The results of these tests will allow your doctor or hair restoration specialist to de-termine if the hair loss could be due to nutritional, hormonal or stress factors.
The doctor will also ask how long the hair loss has
been occurring and whether other women in the family have similar loss. Whether the hair is breaking or falling out at the
Women's Hair Loss 95
roots and if the hair loss is patchy or generalised thinning across the scalp can also help diagnose the cause.
Hair loss in patches can be due to alopecia areata,
which affects around 2% of women. The exact cause of this is unknown, but it is thought to be hereditary or an auto-immune condition.
If excessive hair comes away during brushing, this
could be due to loose anagen syndrome, in which healthy, growing hairs are not held firmly in the follicles and are easily combed out. This condition is most often seen in blonde haired children. Shedding over the entire scalp is a condition called telogen effluvium. In this, an excessive number of hairs are shed simultaneously. This can be a long term chronic condi-tion, or sometimes acute. A stressful event such as a high fe-ver, a severe dietary deficiency or severe blood loss can cause acute diffuse shedding.
Hair can also be pulled out if the hair is usually worn
in tight braids or a tight ponytail. The continual tension pulling on the hair leads to traction alopecia, where the hair is perma-nently lost from the affected follicles.
If someone compulsively pulls or plucks their hair, this
can lead to irregular bald patches. This condition is called trichotillomania. The compulsive behaviour may be entirely unconscious, but can still lead to permanent hair loss.
Irregular bald patches can also be a result of scarring
from wounds or burns, or from medical treatment such as chemotherapy or radio therapy.
A crash diet or chronic protein deficiency in the diet
can lead to hair loss, as can menopause and some oral contra-ceptives. Abnormalities in thyroid function can contribute to hair loss, as can some illnesses, stress or a major operation. Pregnancy leads to hormonal changes which can increase hair growth. When the body returns to normal after child birth, a
96 New Hair Restoration
sudden loss of the extra hair may give the impression of ex-
cessive hair loss.
Treatments Available, Including Hair
Transplant
The treatment of hair loss in women will depend primarily on
the cause and must be discussed with a doctor or hair restora-
tion specialist.
Many products are available to thicken the existing
hair, or camouflage thinning patches of the scalp in the short term. Hairpieces or wigs can also be used and may be the pre-ferred option for widespread or considerable hair loss on the scalp.
Hair loss in women may have hormonal causes. If it is
due to hormonal changes such as in pregnancy or child birth, it will be temporary and will readjust accordingly. In other cases treatment with anti-androgens may be suitable, or simply changing the oral contraceptive, if taken, to one with low an-drogen activity.
Nutritional causes of hair loss can be addressed by diet
changes or nutritional supplements.
For many women, including those with pattern hair
loss due to genetic factors, the use of Minoxidil (Rogaine®) or the HairMax LaserComb® can be very effective treatments. Both have been tested in clinical trials and are approved by the FDA for use in hair loss. Minoxidil is a topical solution ap-plied to the scalp daily. The HairMax LaserComb® is the size of a large hairbrush and is used by simply brushing across the scalp. It allows laser beams to penetrate the scalp and activate the hair follicles, and can improve hair growth and hair condi-tion.
A hair transplant is also an option for some women.
The suitability will depend on the cause and extent of the hair
Women's Hair Loss 97
loss and whether there is sufficient hair density in the donor region.
If hair loss is confined to a small area, such as a reced-
ing hair line in the temples or due to scarring, a transplant of only a few hundred follicles can be sufficient to make a sig-nificant difference to the woman's appearance and self esteem.
The decision on treatment must be made in discussion
between the patient and a doctor or hair restoration specialist. It will depend on the cause and extent of hair loss, the cost of various options and the desired outcome.
Both women and men should be wary of treatments of-
fering ‘miraculous', ‘sensational' or ‘guaranteed' results. Hair loss is a medical condition and requires medical treatment. As in any medical treatment, the results will vary between indi-viduals and the outcome cannot be guaranteed.
Having said this, women should not be discouraged
from seeking medical advice and the numerous benefits to be gained from partial or full hair restoration. Increased hair growth or hair thickness can give an enormous boost to a woman's self confidence and self esteem, and should never be underestimated.
Hair Texture: Diameter and Density
The texture of hair is a result of both thickness of the individ-
ual strands and density of hairs on the scalp. Scalp hair grows
at about 0.6 – 1.25cm per month, and will normally reduce in
thickness and density with age. Hair in an individual person is
at thickest around 20 years, and diminishes thereafter.
The thickness of hair ranges from fine to coarse, and
varies between different ethnic groups and people. Fine hair has a diameter of 50µm (microns) and is most susceptible to breakage. Medium hair is 60-90µm and is the most common. Coarse hair is relatively strong with and is 100µm or more.
98 New Hair Restoration
The density of hair refers to the number of hairs on the
scalp. As each follicle is in a continuous cycle of growth, deg-radation and resting, the number of hairs of a noticeable length will be less than the number of follicles. 50 – 100 hairs are shed normally every day and 10% of follicles will be resting stage at any time.
On average there are 100,000 – 150,000 follicles on
the scalp. If there are fewer than 90,000 hairs on the scalp, the hair density is considered thin. A rough estimate of hair thick-ness can be made by closing your thumb and forefinger around your ponytail. If your fingers form a 1cm circle or smaller, your hair is thin. If they form a circle 2cm or larger, your hair is thick.
There are three major types of ethnic hair: Asian, Afri-
can and Caucasian. People of Asian descent have low density hair, which is coarse and gives the appearance of thick hair. Ethnic African hair has characteristic irregular curling along the length, giving high coverage and high density, yet of fine diameter. Caucasian hair is between these two extremes with great variation. Frequently people with blonde hair have the highest number of follicles and those with red hair have the fewest.
Fine hair can be a consequence and a predictor of thin-
ning hair. People's hair tends to become finer before being lost; Women with thin hair initially are more susceptible to hair loss than those with naturally coarse hair.
For more information visit the website for the Interna-
tional Society of Hair Restoration Surgery - www.ishrs.com - and their articles on hair loss in women:
• Hair Loss and Restoration in Women
Women's Hair Loss 99
• Psychological Effects of Hair Loss in Women
• When is Hair Transplantation an Option for a Woman
with Hair Loss? http://www.ishrs.org/articles/hair-transplants-women2.htm
• "Women and Hair Loss: A Physician's Perspective"
Dr Matt L. Leavitt 2004 Published by Beautiful Media USA www.beautimedia.com
The Ludwig Classification of Female Pattern Hair
Loss.
100 New Hair Restoration
10 Repairing Superseded Techniques.
housands of men and women have undergone hair trans-pl
T ant surgery over the years. These patients now have
permanent hair growing in their once thinning areas. Earlier cases the hair restorations were less advanced than today's technology and surgical techniques.
Earlier chapters detailed and compared various surgi-
cal hair restoration techniques that developed over the years. The objective in sharing this information is to show why there is such a dramatic difference in the appearances of older hair transplants and the new hair transplant.
Plugs
The standard surgical method was a technique that trans-
planted large bunches of hair follicles - known as "plugs"-
from the back of the head to the balding areas. Plugs contained
30 or more hairs, which could not be positioned or angled to
look natural.
Since hair does not grow in evenly spaced rows of
large tufts, it produced noticeably unnatural looking results, sometimes referred to as "Barbie-doll" or "corn-row" hair.
102 New Hair Restoration
Fixing Old-Style Hair Transplants
For "plugs" from earlier years, corrective surgery (plug repair)
and refinements to hairlines are possible.
Hair restoration surgeons skilled in Follicular Unit
Transplant, in combination with an artistic hair grafting ap-proach and some creative ‘recycling' of hair from the tufts, have the ability to help patients to significantly improve the appearance of their previous hair transplant surgery.
The "pluggy" transplant performed a decade earlier shows the
"corn row" appearance.
With Follicular Unit grafts we
were able to fill in the spaces be-
tween the plugs to achieve a
more natural and acceptable ap-
pearance after only one pass.
In some cases removal and recycling of the patient's
plugs is necessary, in addition to transplanting new, smaller grafts around the older transplanted hair. In these procedures, the older, large plugs are partially or entirely removed from the scalp and "recycled". The surgeon divides each plug into much smaller Follicular Unit grafts and then re-implants them into the scalp. Great care and skill is required to create natural angles, the right orientation and position of the transplanted hair.
"Recycled" hair plugs, together with newly harvested
hair transplanted from the back of the head, offer patients with old-style hair restorations a more natural hairline. It is quite common for these patients to achieve a new natural look in only one session.
More Good News
For patients considering ‘hairline refinement' surgery to im-
prove upon their earlier hair restoration results, there has never
been a better time to seek help.
Patients are surprised and happy when they learn that
today's surgical procedures are so much more efficient, effec-tive and comfortable than their earlier transplant surgeries. Post-operative healing is also easier and faster. The natural and undetectable new hairline is certainly the best news.
104 New Hair Restoration
11 Eyebrows and Eyelashes
oss of eyebrow or eyelash hair can make an individual feel ve
L ry self-conscious about his or her appearance and
new hair transplantation techniques can often restore the hair. Many people don't realise the full impact that eyebrows or eyelashes can make on the total facial appearance until you see a person without them.
Hair transplantation has been used successfully for
many years to fill out patchy or absent eyebrows. Eyelash transplantation is a more recent procedure. The procedures should only be performed by a surgeon who has had further specialised training in these techniques
Eyebrow hair loss can occur for several reasons, and is
most commonly associated with the following:
• Physical trauma
• Systemic or local disease
• Over plucking, typically to reshape the eyebrow
• Trichotillomania ,obsessive compulsive plucking
• Medical or surgical treatments like radiation therapy or
• Genetic factors
106 The New Hair Restoration
Eyebrow restoration involves placement of single hairs
in the natural growth pattern of the previous hair. Meticulous placement of several hundred hairs can restore eyebrows.
Eyelash restoration surgery is performed with local
anaesthesia and involves the transplantation of 20 to 25 spe-cially prepared grafts to each upper eyelid using a technique that I have developed. Donor hair is taken from the back of the head and the grafts are trimmed very fine. The new lashes grow longer than usual and must be cut regularly. Eyelash re-construction elevates patients' self-esteem.
Before After
For more information, visit the website for the Interna-
tional Society of Hair Restoration Surgery - www.ishrs.com - and specifically their article on eyelash transplantation: http://www.ishrs.org/articles/eyelash-transplantation.htm
he main advantages of Follicular Unit Transplantation are
T greater hair coverage, more natural appearance with unde-
tectable surgery.
Options available and the results of the latest tech-
niques in hair transplant surgery have been described. How-ever it is important to seek expert advice as results do vary from person to person depending on hair characteristics, gen-eral health and other unknown factors. It is wise to thoroughly research a surgeon's credentials before committing to a hair transplant.
Check whether the surgeon is a member of the Interna-
tional Society of Hair Restoration Surgery (ISHRS) and whether they work full or part time in hair restoration. Also check whether they will actually perform all of the procedure themselves, and ask what techniques they use. How will they harvest the donor hair and how will the hair follicles be trans-planted into the recipient areas? Will the surgeon achieve a natural looking hairline as in the ‘snail track'? Will they achieve hair density in thinning areas? Ask if you can see pho-tos or speak to former patients.
Think about your expectations and discuss these in de-
tail with the hair restoration specialist. Are you looking for treatment for short, medium or long term results?
108 The New Hair Restoration
If you are not convinced that the clinic you visit meets
the strict standards you feel are required to give you the best results, go elsewhere. This is a major decision on your part that requires research. Obtain the best possible hair restoration advice and treatment. The results of hair transplant surgery are permanent. To avoid the possibility of costly corrective treat-ment later, care should be taken to make an informed initial decision.
Reputable hair transplant surgeons are members of
ISHRS (International Society of Hair Restoration Surgery). You can visit the society's website for reliable information: www.ishrs.org - International Society of Hair Restoration Surgery
13
Hair Transplantation
Q & A
Q. What is hair transplantation or hair restoration sur-
gery?
A. Hair transplantation is also referred to as hair restoration
surgery. It is considered to be a minor, outpatient surgical pro-
cedure. It involves transplanting grafts of hair follicles that
always grow hair (this is the hair located toward the base of
the back of the scalp) into the areas affected by hair thinning
or loss.
Q. Can you use someone else's hair for my transplant?
A. No, because as "foreign tissue" it would be rejected by your
body.
Q. Does your clinic still use "plug" transplants?
A. No. The plug technique was the method used for hair trans-
plant surgery from the 1950's through the 1980's. Plugs con-
sisted of larger tufts with as many as thirty hairs. Today, ad-
vanced surgical techniques allow us to use Micro Grafts, con-
sisting of only 1-4 hairs. Follicular Unit grafts used today are
far superior to the old plug method.
110 New Hair Restoration
Q. Why doesn't the hair that is transplanted fall out?
A. While they may look identical, the hairs used in transplan-
tation are genetically different from the hairs that fall out in
pattern baldness. These is why sufferers of androgenic alope-
cia (Male Pattern Baldness) usually lose hair at the front and
top of the head, but retain the hair that grows on the sides and
back of the head.
Q. Won't the bald area kill the new grafts?
A. The previously bald area does not "poison" the transplanted
grafts; this is a common misconception. The fact that the
transplanted hair follicles have been moved from one area of
the scalp to another has no effect on their genetic predisposi-
tion to grow hair.
Q. Is a hair transplant painful?
A. New advances in the field of hair restoration surgery pro-
vide a relatively pain-free experience for today's patients.
During the procedure, patients require only a mild anaesthetic
to minimise discomfort. Following surgery, many patients
need nothing more than paracetamol for a few days. In fact
many patients take no medication afterwards.
Q. Is a patient awake during transplantation surgery?
A. Patients are given a mild sedation. The patient drifts in and
out of sleep during the procedure and the scalp is numb due to
anaesthetic for the duration of the surgery.
Q. What about general anaesthesia?
A. No, general anaesthesia is unnecessary for this procedure.
Hair Transplantation Q&A 111
Q. How much time does it take?
A. Follicular Unit hair transplants often take several hours de-
pending on how many units will be implanted. Mega-sessions
can take more than five hours. The length of time depends on
the special procedure involved and the area of implant place-
ment.
Q. Will I miss work or need time off after surgery?
A. Patients will not be able to drive or operate machinery for
24 hours after surgery due to the sedation. I recommend hav-
ing 3 days relaxation after the procedure.
Q. What about my exercise program following surgery?
A. It is best to avoid any strenuous exercise for up to a week
following surgery. Ease into your exercise program by cutting
the time you normally do to half, then gradually over two to
three weeks resume your normal pace.
Q. Will I be able to wear my hairpiece after surgery?
A. Yes, after the first three days during which time the recipi-
ent sites should be kept dry. From then on, we advise patients
to do without it as much as possible for the purposes of
quicker healing and hair growth. It is also easier to complete
the transition out of a hairpiece when a patient can learn to
become less dependent on it. Rubbing from the hairpiece has
been reported anecdotally as interfering with hair growth.
Q. Are the hairs long immediately after the transplant?
A. No. Typically, the transplanted hairs are only a few milli-
metres in length immediately following surgery. During the
first fortnight, nearly all of the newly transplanted hairs will
fall out. This is normal. It takes approximately 3-4 months fol-
lowing this initial shedding for new hair growth to begin.
112 New Hair Restoration
Q. How long will it take before my hair starts to grow
permanently?
A. You can expect to see normal, permanent hair growth 3-4
months following transplantation. The normal rate of hair
growth ranges from 0.6 – 1.25cm per month. The full result
will require 6-12 months to be appreciated. Sometimes growth
can be delayed for 18-24 months for reasons unknown.
Q. Can I perm, colour or dye my new hair?
A. Yes, you can. The transplanted hair is your own hair, and
can be cut, coloured and styled as normal after 2 weeks.
Q. What about insurance?
A. Usually insurance does not cover elective surgical proce-
dures. If it is accident or health related, than you will likely
have some, if not all covered.
Q. When is the best time to have my transplant?
A. While most men and women who have begun to notice hair
loss can benefit from hair restoration, not all patients are can-
didates for surgical hair transplantation. For some men it is
possible to stop or even reverse the progression of hair loss
with medical therapies such as Rogaine®, Propecia® or
HairMax LaserComb®. Rogaine® and HairMax LaserComb®
are also effective non-surgical treatments for women.
Q. At what age should a person consider hair restoration?
A. Medical and surgical hair restoration can be safely and ef-
fectively performed on healthy patients of all ages. Typically,
the youngest patients are in their twenties while the majority
of patients range in age from mid-thirties to mid-sixties.
Hair Transplantation Q&A 113
Since pattern hair loss, the most common form of hair
loss, is irreversible without medical intervention, patients can retain more of their hair if they act early.
Mimicking nature—The gold Standard in New Hair Restora-
tion.
114 New Hair Restoration
5-Alpha-reductase
5-alpha-reductase is the enzyme which converts testosterone
to dihydrotestosterone (DHT), the hormone that triggers An-
drogenic Alopecia in individuals who are genetically suscepti-
ble. Type 1 5-alpha-reductase is found primarily in the skin
and 5-alpha-reductase Type 2 is found primarily in the pros-
tate and inner sheath of the hair follicle.
Alopecia
Complete or partial lack of hair resulting from various condi-
tions.
Alopecia Areata
Alopecia Areata is the medical term for hair loss which occurs
in patches on the scalp.
Alopecia Totalis
This is the complete loss of scalp hair often combined with the
loss of eyebrows and eyelashes.
Alopecia Universalis
Alopecia Universalis is the term for hair loss which occurs
over the entire body.
Anagen
This is the term for the growing phase of the hair cycle which
lasts five - seven years in a healthy person.
Androgenic Alopecia
This term is the common name for male or female pattern
baldness which depends on the genetic predisposition of the
hair follicles and the levels of androgen in the body.
116 New Hair Restoration
Androgens
Androgens are male sex hormones.
Anti-androgen
An anti-androgen blocks the effects of androgens, normally by
blocking the receptor sites.
Catagen
This is the end of the active growth period of a hair follicle,
and is marked by changes in the follicle.
Cicatricial Alopecia
This is baldness due to scarring. The follicles are absent in
scar tissue.
Coronal angled grafting (a.k.a. lateral grafts)
Grafts are placed into recipient sites made with a very small
rectangular blade that pierces the skin at right angles to the
hair direction.
Crown
Area at the top of the head.
Cyproterone Acetate
Cyproterone Acetate is an anti-androgen. It is prescribed to
treat hirsutism and androgenic alopecia in women.
Dermal papilla
The dermal papilla is situated at the base of the hair follicle.
The dermal papilla contains nerves and blood vessels which
supply glucose for energy and amino acids to make keratin.
DHT (5-alpha dihydrotestosterone)
DHT is a male hormone that is suggested to be the main cause
for the miniaturization of the hair follicle and subsequent hair
References/Notes 117
loss. DHT is formed from the male hormone testosterone by
the enzyme 5-alpha-reductase.
Donor Site
Site where hair follicles are harvested during transplant sur-
gery.
Dutasteride
A medication for the treatment of benign prostatic hyperplasia
(BPH); It is an inhibitor of type 1 and type 2 5-alpha-reductase
enzymes responsible for converting testosterone to DHT.
Finasteride
Finasteride is the generic name of a drug that binds with 5-
alpha-reductase type 2 enzyme to reduce the amount of DHT
in the prostate and serum. Finasteride is approved by the FDA
for treatment of benign prostatic hyperplasia (BPH) as Pro-
scar® 5mg daily dose and hair loss as Propecia® 1mg daily
dose.
Follicle
The follicle is a tube-like structure in the skin in which devel-
ops a hair shaft.
Follicular Unit
Groupings of 1 to 4 hairs that grow together.
Follicular Unit Transplantation
A recent technique in hair transplantation where the naturally
occurring follicular units of hair follicles are implanted as a
natural group.
Gene Therapy
Gene therapy is a treatment method which involves the ma-
nipulation of the genetic makeup.
118 New Hair Restoration
Hair Cloning
A technique under development which could make an unlim-
ited crop of donor hair available for transplanting.
Hair-A-Gain®
A brand name for Minoxidil.
Ludwig Scale
Classification of female pattern hair loss.
Medulla
The medulla is a central zone of cells usually only present in
large, thick hairs.
Micro Graft
A very small hair graft usually consisting of one or two folli-
cles.
Mini Graft
A small hair graft usually consisting of between three to ten
hair follicles.
Minoxidil
Minoxidil is the generic name of the brand name drug Ro-
gaine®. Minoxidil is a topical lotion available over-the-
counter in 2% to 5% solution. Minoxidil was the first drug to
be approved by the FDA for the treatment of androgenic
alopecia.
Norwood/Hamilton Scale
The most commonly used scale for the classification of male
pattern hair loss.
Papilla
Knoblike indentation at the bottom of the follicle which con-
tains a vascular loop for nourishment.
References/Notes 119
Propecia®
A brand name for Finasteride 1mg, approved for the treatment
of male pattern hair loss.
Proscar®
The brand name for Finasteride 5mg, approved for the treat-
ment of benign prostatic hyperplasia (BPH).
Punch Graft
The old fashioned way of removing grafts for hair transplants,
usually carried out using an instrument called a trephine.
Recipient Site
The bald or thinning area into which hair grafts or plugs are
transplanted.
Rogaine® and Hair-A-Gain®
Brand names for Minoxidil, a topical lotion for the treatment
of hair loss.
Sagittal Angled Grafting
Grafts are placed into recipient sites made with a very small
rectangular blade that pierced the skin parallel to the hair di-
rection.
Saw Palmetto
Saw Palmetto is a plant native to North America. It may have
some, unproven therapeutic benefits for benign prostatic hy-
perplasia (BPH). It does not lower DHT or testosterone levels
and has never been shown to increase hair growth.
Sebaceous glands
These are sebum (oil) producing glands found in the skin
throughout the body except in the palms of the hands and soles
of the feet.
120 New Hair Restoration
Snail Track Technique
A term coined by Dr Martinick to describe the irregular out-
line of the hairline giving a more natural appearance.
Spironolactone
This drug acts as an anti-androgen and is used in the treatment
of androgen related disorders such as female pattern baldness
and hirsutism.
Telogen
The resting phase of the hair cycle.
Testosterone
A predominantly male hormone which promotes the develop-
ment of male characteristics.
Topically
Applied directly onto the skin.
Traction Alopecia
This refers to hair loss which occurs due to traction being
placed on hair. Traction alopecia is commonly seen with
braids, pony tails and other hairstyles which cause tension on
the scalp.
Transection
Damage to hair follicles that can decrease survival after trans-
plantation.
Trichotillomania
A compulsion to pull out one's own hair.
Vellus
The soft downy hair found covering the body.
References/Notes 121
Vertex
The top of the head towards the posterior position, including
the area at which the hair grows in a spiral pattern.
122 New Hair Restoration
References/Notes
Notes to Pages Page 1 Note 1
• Budd, D & Himmelberger, D, et al. (2000). ‘The ef-
fects of hair loss in European men: a survey in four countries.' European Journal of Dermatology, 10(2): 122-7.
• ‘Samson syndrome – UK survey reveals how hair loss
directly affects self worth' (2006). PR Newswire/boots. http://hairloss.about.com/b/2006/09/12/samson-syndrome-uk-survey-reveals-how-hair-loss-directly-affects-self-worth.htm.
• Pertschuk, M & Trisdorfer, A, (2004). ‘Men's bodies –
the survey'. Psychology Today Magazine, Sussex Pub-lishers, L.L.C, NewYork. http://psychologytoday.com/articles/index.php?term=19941101-000022&page=1.
Page 1 Note 2
• Whiting, D.A, (2001). ‘Advances in the treatment of
male androgenetic alopecia: A brief review of Finas-teride studies' European Journal of Dermatology, 11(4): 332-4.
References/Notes 123
Page 17 Note 3
• Heyman, E.R. (2005). ‘A Randomized, Double-blind
Clinical Trial to Evaluate the Safety and Efficacy of the HairMax LaserComb for the Treatment of Andro-genetic Alopecia in Males'. Lexington International, L.L.C., Boca Raton.
Page 18 Note 4
• Kaufman, K.D, Olsen, E.A, Whiting, D, et al. (1998).
‘Finasteride in the treatment of men with androgenetic alopecia. Finasteride male pattern hair loss study group.' J Am Acad Dermotol, 39:578-89.
• Leyden J, Dunlap F, Miller B, et al. (1999). ‘Finas-
teride in the treatment of men with frontal male pattern hair loss.' J Am Acad Dermotol, 40:930-37.
Page 19 Note 5
• Kaufman, K.D, Olsen, E.A, Whiting, D, et al. (1998).
‘Finasteride in the treatment of men with androgenetic alopecia. Finasteride male pattern hair loss study group.' J Am Acad Dermotol, 39:578-89.
• Leyden, J, Dunlap, F, Miller, B, et al. (1999) ‘Finas-
teride in the treatment of men with frontal male pattern hair loss.' J Am Acad Dermotol, 40:930-37.
• ‘Propecia product information.' (2008), MERCK &
CO., Inc., Whitehouse Station, NJ, USA. http://www.propecia.com
124 New Hair Restoration
Page 56 Note 6
• Martinick, J & Rassman, W. (2002) FUE Rebuttal,
ISHRS, Chicago, www.martinick.com.au
• Rassman, W. (2006) ‘What Doctors don't want you to
know about FUE'. BaldingBlog.com. http:www.baldingblog.com
• Rassman, W & Bernstein, R, et al. (2002), ‘Follicular
Unit Extraction: minimally invasive surgery for hair
transplantation.' Dermatologic Surgery 28: 720-728
• Martinick, J. (2004) ‘The latest developments in surgi-
cal hair restoration'. Facial Plastic Surgery Clinics of
North America 12(2): 249-252.
• Unger, W & Shapiro, R. (2004), ‘Hair Transplanta-
tion'. Informa Health Care, New York.
Page 92 Note 7
• Price, V. (2003), ‘Androgenetic Alopecia in Women'
JID Symposium Proceedings. 8:24-27
• Price, V. (1999), ‘Treatment of Hair Loss' The New
England Journal of Medicine. 341(13): 964-973
• Olsen, E. (2001), ‘Female pattern hair loss' Journal of
the American Academy of Dermatology 45(3)S70-80
References/Notes 125
Additional Information
Contact Details
Telephone:
[email protected]
www.martinick.com
Other useful websites may include the following:
International Society of Hair Restoration Surgery www.ishrs.org Objective information on hair loss and treatments: www.hairlossinfo.com.au
Information on hair transplants; Balding Blog: www.iahrs.org , www.baldingblog.com Information on hair loss: www.hairlosshelp.com Or search on Google for Dr. Jennifer Martinick
Source: http://www.martinick.com/wp-content/uploads/new-hair-restoration-ebook.pdf
Takeda Receives Simultaneous European Marketing Authorization for Three New Type 2 Diabetes Therapies, VipidiaTM (alogliptin) and Fixed-Dose Combinations VipdometTM (alogliptin and metformin) and IncresyncTM (alogliptin and pioglitazone) Osaka, Japan, September 24, 2013 – Takeda Pharmaceutical Company Limited (Takeda) today announced that the European Commission has granted Marketing Authorization (MA) for VipidiaTM (alogliptin), a dipeptidyl peptidase IV (DPP-4) inhibitor, for the treatment of type 2 diabetes patients who are uncontrolled on existing therapies1-3and for the fixed-dose combination (FDC) therapies VipdometTM (alogliptin with metformin) and IncresyncTM (alogliptin with pioglitazone). The Committee for Medicinal Products for Human Use (CHMP), of the European Medicines Agency (EMA), issued a positive opinion for these products on July 26, 2013.
Thermo Scientific iCAP 7000 Series ICP-OES The new Thermo Scientific™ iCAP™ 7000 Series ICP-OES provides the lowest cost multi-element analysis for measuring trace elements in a diverse sample range, combining advanced performance with high productivity and ease of use. The instrument provides your environmental, pharmaceutical, industrial or food safety facility with the lowest cost of analysis per sample, producing consistently reliable data, whilst ensuring compliance to global regulations and standards.