Whole-body vibration improves walking function in individuals with spinal cord injury: a pilot study

G ModelGAIPOS-2815; No of Pages 5
Gait & Posture xxx (2009) xxx–xxx
Contents lists available at
Whole-body vibration improves walking function in individualswith spinal cord injury: A pilot study
Lanitia L. Ness ,Edelle C. Field-Fote
a The Miami Project to Cure Paralysis, University of Miami Miller School of Medicine, Miami, FL, USAb The Department of Physical Therapy, University of Miami Miller School of Medicine, Miami, FL, USAc The Department of Biomedical Engineering, University of Miami, Coral Gables, FL, USA
Injury to the central nervous system often results in impairments that negatively affect walking function.
Received 28 January 2009
Prior evidence suggests that vibration may improve walking function. The purpose of this study was to
Received in revised form 20 May 2009
determine whether repeated use of whole-body vibration (WBV) is associated with improvements in
Accepted 26 June 2009
walking function in individuals with spinal cord injury (SCI). Subjects were 17 individuals with chronic(�1 year), motor-incomplete SCI. Subjects were tested before and after participation in a 12-session (3
days/week for 4 weeks) intervention of WBV. We assessed change in walking function via 3D motion
capture, with walking speed as the primary outcome measure. We also assessed the influence of the
WBV intervention on secondary gait characteristics, including cadence, step length, and hip-knee
Afferent inputHuman movement system
intralimb coordination. Walking speed increased by a mean of 0.062 � 0.011 m/s, a change that wasstatistically significant (p < 0.001). The WBV intervention was also associated with statistically significantincreases in cadence, and both the stronger and weaker legs exhibited increased step length and improvedconsistency of intralimb coordination. Changes in cadence and step length of the stronger leg were stronglycorrelated with improvements in walking speed. The improvement in walking speed observed with the WBVintervention was comparable to that reported in the literature in association with locomotor training. Thismagnitude of change has been identified as being clinically meaningful, even in non-clinical populations.
These findings suggest WBV may be useful to improve walking function with effects that may persist forsome time following the intervention.
ß 2009 Elsevier B.V. All rights reserved.
of vibration placement and direction of progression Inindividuals with Parkinson's disease, vibration applied through
Loss of walking function is a common consequence of spinal
the soles of the feet during walking increases walking distance,
cord injury (SCI), and for these individuals, regaining walking
speed, stride length, and improves stride variability Vibration
function is a high priority Individuals with SCI, and other
may also excite spinal circuitry (i.e., locomotor pattern generators)
populations with disorders of the central nervous system, often
involved in the production of locomotor output .
have various impairments that negatively impact walking func-
Whole-body vibration (WBV) is increasingly being used in
tion. For example, muscle weakness and sensory impairment
elderly individuals and in clinical populations In
result in reduced levels of muscle activation and decreased walking
individuals with SCI, our studies offer preliminary evidence that a
speed . Spasticity may result in altered muscle timing and co-
12-session intervention of WBV decreases spasticity of the
contraction associated with spastic gait patterns Decreased
quadriceps muscles . The use of WBV has also been associated
walking function results from any one, or a combination, of these
with changes in walking function Elderly individuals
who received a 2-month WBV intervention in combination with
In non-disabled (ND) individuals, vibration to the muscle body
balance, muscle strengthening, and walking exercises demon-
or tendon increases walking speed, depending on the combination
strated increased walking speed and step length compared toindividuals who did the same exercise program without WBV In individuals with Parkinson's disease, a 3-week intervention ofWBV is associated with improvements in walking speed In
* Corresponding author at: The Miami Project to Cure Paralysis, University of
adults with spastic diplegia due to cerebral palsy, an 8-week
Miami Miller School of Medicine, 1095 NW 14 Terr (R-48), Miami, FL 33136, USA.
intervention of WBV is associated with improvements in muscle
Tel.: +1 305 243 7119; fax: +1 305 243 3913.
E-mail address: (E.C. Field-Fote).
strength and reductions in spasticity of the knee extensor muscles,
0966-6362/$ – see front matter ß 2009 Elsevier B.V. All rights reserved.
doi:
Please cite this article in press as: Ness LL, Field-Fote EC. Whole-body vibration improves walking function in individuals with spinalcord injury: A pilot study. Gait Posture (2009), doi:

G ModelGAIPOS-2815; No of Pages 5
L.L. Ness, E.C. Field-Fote / Gait & Posture xxx (2009) xxx–xxx
but the distance walked in 6 min was unchanged In
parameters. Information about daily use of medications and assistive devices for
individuals with SCI who were unable to stand without long-leg
mobility was also recorded.
Demographic data for the subjects are given in All subjects gave written
braces, a case series published in an abstract attributed the use of
and verbal informed consent to participate in a protocol approved by the Human
WBV with the progression of function from standing to walking
Subjects Research Office at the institution. All subjects were instructed to maintain
. Evidence of the effects of WBV on walking function is limited
their regular exercise and medication habits until completion of the study.
in individuals with SCI.
The purpose of this study was to determine whether repeated
2.1. WBV intervention
use of WBV is associated with improvements in walking function,
Subjects received an intervention consisting of WBV (Power Plate; Northbrook,
as defined by changes in walking speed, in individuals with
IL) 3 days/week for 4 weeks. Each session included four 45-s bouts with 1 min of
chronic, motor-incomplete SCI. In individuals with SCI, increased
seated rest without vibration between bouts according to previously published
walking speed is a standard benchmark for improvement in
protocols (. During each WBV bout, subjects stood on the vibrationplatform with knees flexed approximately 308 from anatomical neutral. Vibration
walking function In addition, we assessed changes in
was delivered at 50 Hz with a vertical displacement of 2–4 mm (depending on
secondary gait parameters including step length, cadence, and
subject weight).
consistency of hip-knee intralimb coordination. Our prior studiesof interventions to improve walking function in individuals with
2.2. Testing procedure
SCI have focused on locomotor training or nutrient
The effects of the 12-session WBV intervention on walking function were
supplementation While there is preliminary evidence in that
quantified by comparing the kinematic data acquired prior to the intervention
WBV may improve walking function in elderly individuals and
(initial test) to that collected within 7 days of the last WBV session (final test). One
individuals with Parkinson's disease , there are no published
subject returned an additional time at 5-week post-WBV for a follow-up test
studies related to the influence of WBV on walking function in
session to allow assessment of persistence of intervention effects. An array of 21
individuals with SCI, many of whom have a limited ability to
reflective markers were placed bilaterally at the lateral malleoli, 5th ray metatarsal-phalangeal joints, heels, lateral knee joints, greater trochanters, anterior superior
maintain standing. Based on the prior evidence, we hypothesized
iliac spines, shoulders, elbows, and wrists as well as at C7, T10, and the sacrum.
that the 12-session intervention of WBV would be associated with
Kinematic data were collected using an 8-camera 3D motion capture system (Peak
improvements in walking speed and the secondary gait para-
Motus1 Software, Peak Performance, Centennial, CO). Recording of kinematic data
meters. In this consideration-of-concept study , our goal was to
was performed in a calibrated space with data captured at 60 Hz.
For each walking test session, subjects walked five times across a 10-m walkway
determine whether there was value in pursuing this line of study,
at their preferred walking speed; subjects were allowed to rest between walking
and whether it was feasible to use WBV in individuals with SCI
tests. During each walking test, subjects were given 30 s to complete the 10-m walk,
relative to subject tolerance and incidence of adverse events.
and all outcome measures were extracted from data captured within the central6 m of the walkway. Subjects used assistive devices as required during testing.
Fourteen subjects used a rolling walker, one subject did not have the necessary
2. Subjects and methods
hand function to grip the handles of a standard rolling walker and performed the
Seventeen subjects (3 women and 14 men; age 28–65) with SCI enrolled in the
test using a rolling walker with bilateral forearm platform supports, and two
study. All subjects underwent clinical examination prior to testing. Subject
subjects did not require assistive devices. If a subject required an assistive device,
inclusion criteria were motor incomplete, chronic (�1 year duration) SCI, and
the same device was used both for the initial and final test sessions.
ability to rise from sitting to standing with no more than moderate assistance fromone person, and ability to stand (using upper extremity support) for at least 1 min.
2.3. Data analysis and statistics
American Spinal Injury Association (ASIA) motor and sensory scores , and ASIAImpairment Scale (AIS) classification were evaluated by a physical therapist
Statistical Analysis Software 9.1.3 (Cary, NC) was used for all statistical analyses.
who was not otherwise involved in the study. All individuals had asymmetrical
All data were checked and met the parametric assumptions of homogeneity
lower extremity motor scores that were used to identify the weaker and stronger
(Levene's test for equality of variances) and normality (Kolmogorov–Smirnov Z-
extremity. Subject height was recorded for the purpose of normalizing gait
test). Significance was set at a = 0.05. Walking speed (SPEED; meters/second; m/s)
Table 1Demographics of participants, LEMS = lower extremity motor scores represent the sum of the motor scores for the five key muscles of both legs graded according to ASIAguidelines prior to the WBV intervention.
Antispastic agents
Primary daily assistive device
Personal transporter
Fig. 1. Procedure for a single session of whole-body vibration (WBV). Each session of WBV consisted of four bouts of WBV at a frequency of 50 Hz and an intensity of 2–4 mm(depending on the subject weight). Each vibration bout was separated by a period of 1 min seated rest.
Please cite this article in press as: Ness LL, Field-Fote EC. Whole-body vibration improves walking function in individuals with spinalcord injury: A pilot study. Gait Posture (2009),
G ModelGAIPOS-2815; No of Pages 5
L.L. Ness, E.C. Field-Fote / Gait & Posture xxx (2009) xxx–xxx
was calculated from the distance traversed in the direction of forward progressionas measured from the sacral marker. A one-tailed, paired t-test was used to comparethe mean speed of the five walking trials from the initial and final test sessions. Aconvenience sample of one participant (selected because he lived locally) returnedfor a follow-up walking test session 5-week after the last session of WBV. Walkingspeed for this subject was compared to both the initial and final tests to assesspersistence of change in speed associated with the WBV intervention.
Gait parameters were calculated from the kinematic measures. Data were
filtered using a Butterworth filter with a 6 Hz cutoff. Bilateral step lengths wereextracted from the coordinates of the heel in the direction of progression. Steplengths (m) were determined by the distance between two consecutivecontralateral heel strikes, and normalized to subject height. A one-tailed, pairedt-test was used to compare the mean initial and final test values of the strong legstep length (SSL) and weak leg step length (WSL). Cadence (CAD; steps/min) wascalculated by dividing the total number of steps by the time needed to complete the
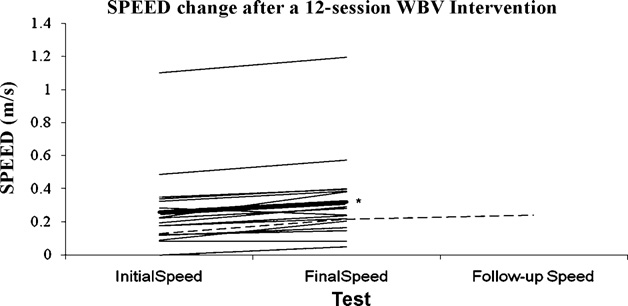
Fig. 2. All subjects change in walking speed (SPEED; mean � standard error)
steps. A one-tailed, paired t-test was used to compare the mean CAD of the initial
associated with 12-session whole-body vibration (WBV) intervention. Change in
and final tests. The values of SSL, WSL and CAD are directly derived from a single
SPEED values for all subjects (thin lines) and group mean change (thick line). Group
reflective marker and may therefore be expected to be interrelated, therefore a
mean initial SPEED value (0.259 � 0.248 m/s) and final SPEED value (0.321 � 0.260 m/
Bonferroni correction was used to adjust the alpha level for four pair-wise (SPEED,
s) were significantly different (*). The y-axis has been broken from 0.6 m/s to 1 m/s
CAD, SLL, and WSL) comparisons resulting in a corrected value of a = 0.0083.
because there were no SPEED values measured in this range. One subject returned for a
Intralimb coordination was defined as the ability to produce a consistent
follow-up test 5-week (dashed line) after the last WBV session, had an initial SPEED of
relationship of hip-angle-to-knee-angle coupling over multiple step cycles
0.128 m/s, a final SPEED of 0.215 m/s and a 5-week follow-up SPEED of 0.241 m/s.
The hip angle was defined by the trunk and thigh segments. The knee angle wasdefined by the thigh and shank segments. Vector coding was used to quantifyintralimb coordination wherein the angular component of the coefficient ofcorrespondence (ACC) represents the degree of consistency of the hip-kneerelationship over multiple cycles . It has been suggested that ACC valuesoffer insights into the organization of control mechanisms (i.e., locomotor centralpattern generators) underlying coordination of innate, cyclic behaviours Inindividuals with SCI, changes in the ACC value correlate well with changes inwalking speed associated with locomotor training . ACC was calculated for boththe strong ACC (SACC) and weak ACC (WACC) legs. An increase in ACC value frominitial to final was interpreted as increased consistency of intralimb coordination. Aone-tailed, paired t-test was used to compare the mean SACC and WACC valuesfrom the initial and final tests.
To determine which gait parameters were most closely associated with changes
in walking speed, Pearson correlations where used to identify the relationshipbetween SPEED and the parameters of CAD, SSL, WSL, SACC, and WACC. Pearson rvalues were interpreted as follows: 0.00–0.25 was considered little or norelationship, 0.25–0.50 was considered a fair relationship, 0.50–0.75 wasconsidered a moderate relationship, and 0.75–1.0 was considered to be a goodto excellent relationship .
The pooled standard deviation and Cohen's d was used to calculate the effect size
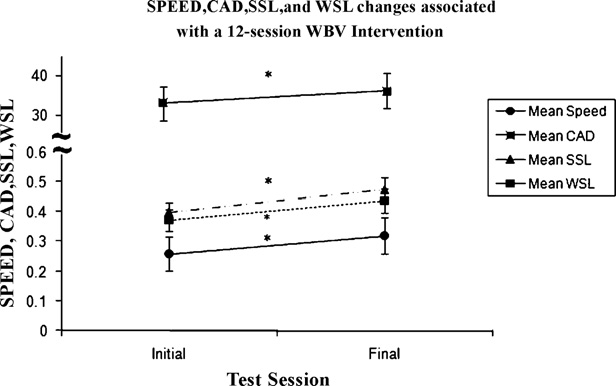
Fig. 3. Group mean changes in walking speed (SPEED; m/s), change in walking
of the change in SPEED associated with use of the WBV intervention.
cadence (CAD; steps/min), and change in weak (WSL) and strong (SSL) step lengths(m) after a 12-session whole-body vibration (WBV) intervention. CAD, WSL and SSLsignificantly decreased (*) after the 12-session intervention of WBV. These gaitparameters contributed to the increase in SPEED. The y-axis values are dependent
on the reported measure and are denoted as group mean � standard error bars. Notethe break in the y-axis from 0.5 to 30 to accommodate for values of cadence.
The group mean walking speed (SPEED) increased by
0.062 � 0.011 m/s (mean � standard error) (from 0.259 � 0.248 m/
non-significant, weak, direct correlation with WSL (r = 0.154,
s in the initial test to 0.321 � 0.260 m/s in the final test), an increase
p = 0.554), SACC (r = 0.018, p = 0.946), and WACC (r = 0.204,
that was statistically significant (p < 0.001) but considered a small
effect size (d = 0.249).
All subjects tolerated the 12-session of WBV, were able to
Subject 16, who returned for a follow-up test 5-week after the
maintain the standing posture for the 45-s bouts of WBV, and
last WBV session, had an initial SPEED of 0.128 m/s, a final SPEED of
reported no adverse effects. These results suggest that it is feasible
0.215 m/s and a 5-week follow-up SPEED of 0.241 m/s. SPEEDvalues of all subjects, group mean, and subject 16 are illustrated in
The 12-session intervention of WBV was also associated with a
statistically significant increase in CAD (from 33 � 5 steps/min[initial] to 36 � 5 steps/min [final]; p = 0.002). SSL significantlyincreased (from 0.194 � 0.090 m [initial] to 0.23 � 0.063 m [final],p = 0.006) and WSL significantly increased (from 0.180 � .082 m[initial] to 0.212 � 0.075 m [final], p = 0.003). The relationshipbetween change in SPEED to changes in, CAD, SSL, and WSL areillustrated in .
There was a statistically significant change in SACC (from
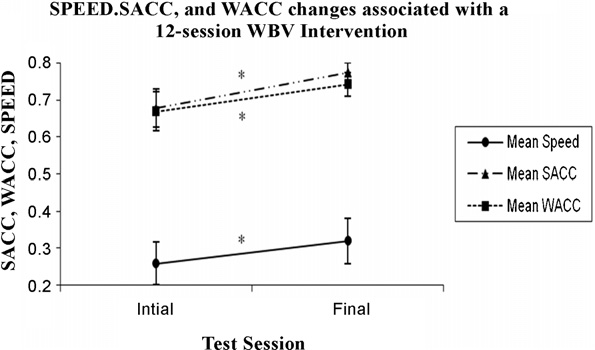
0.68 � 0.22 [initial] to 0.77 � 0.12 [final], p = 0.018) and in WACC(from 0.67 � 0.22 [initial] to 0.74 � 0.14 in [final], p = 0.026). Therelationship between change in SPEED to changes in SACC and WACC
Fig. 4. Group mean changes in walking speed (SPEED; m/s) and the change in strong
is illustrated in .
(SACC) and weak (WACC) coefficients of correspondence (ACC) after a 12-sessionwhole-body vibration (WBV) intervention. The y-axis values are dependent on the
Changes in SPEED had a significant, moderate, direct correlation
reported measure and are denoted as group mean � standard error bars. Note the
with CAD (r = 0.528, p = 0.029), and a non-significant, fair, direct
break in the y-axis from 0.4 to 0.7 because no values were reported in this range. SACC
relationship with SSL (r = 0.344, p = 0.176). Changes in SPEED had a
and WACC significantly decreased (*) after the 12-session intervention of WBV.
Please cite this article in press as: Ness LL, Field-Fote EC. Whole-body vibration improves walking function in individuals with spinalcord injury: A pilot study. Gait Posture (2009), doi:
G ModelGAIPOS-2815; No of Pages 5
L.L. Ness, E.C. Field-Fote / Gait & Posture xxx (2009) xxx–xxx
to use WBV as an intervention in future randomized, controlled
speed. The improvements in walking speed and step length are
studies that assess interventions to improve walking function in
consistent with increases in stride length reported in individuals
individuals SCI. All subjects adhered to the study protocol and
with Parkinson's disease during vibration . However, this is
completed the intervention; many of these individuals indicated
contrary to evidence in ND individuals wherein no change in stride
they would like to continue with these sessions and would be
length during walking was observed with vibration applied to
interested in participating in future studies involving WBV.
tibialis anterior, triceps surae, biceps femoris, rectus femoris, orquadriceps femoris Changes in stride length may not be
evident in ND individuals because their strides are relatively longercompared to individuals with a neuropathology. For this reason,
Our results indicate that consistent use of WBV is associated
individuals with neuropathology may have a larger margin for
with an increase in walking function, as defined by walking speed,
vibration-induced improvement of spatial walking characteristics
in individuals with SCI who have some ability to maintain
compared to ND individuals.
voluntary standing. While the lack of a control group, the inclusion
The degree of consistency of the hip–knee intralimb coordina-
of individuals with varying degrees of walking ability, and the fact
tion of both legs improved, and the improvement was comparable
that it was not possible to blind subjects to the intervention limits
to those observed in a 3-month locomotor training wherein the
the conclusions that can be drawn from these findings, the fact
ACC values improved from 0.56 before to 0.65 after locomotor
remains that the observed changes in walking speed associated
training However, unlike that prior study wherein the change
with WBV were equivalent to those reported for studies of
in intralimb coordination was associated with the change in
locomotor training . In individuals with SCI who participated in
walking speed, in the present study the change walking speed was
a 3-month 5-day/week locomotor training intervention, walking
only weakly correlated with the change intralimb coordination.
speed changes of 0.023 m/s, 0.05 m/s, 0.05 m/s, and
Contrary to our findings, in ND individuals, bilateral Achilles
were associated with manually assisted treadmill training,
tendon vibration did not change walking speed or leg inter-
stimulation-assisted treadmill training, overground training, and
segmental coordination Also in ND individuals, changes in
robotic-assisted treadmill training, respectively. It is possible that
intralimb ankle–knee coordination were not found with vibration
participation in a study made the subjects more conscientious of
applied to tibialis anterior, triceps surae, biceps femoris, rectus
their walking performance or that the pre-, post-test design
femoris, or quadriceps femoris . Our findings and other
increased familiarity with the test, resulting in an improvement.
evidence in individuals with SCI suggest that the consistent
However, we feel these explanations are unlikely, especially in
use of afferent input improves the motor output of the control
light of comparisons to the locomotor training literature . In
mechanisms that have been impaired after a SCI.
healthy elders, a change in walking speed of 0.05 m/s (with asimilar effect size [d = 0.2]) has been judged to be a clinically
5. Implications for function
meaningful change . As illustrated in , 10 out of 17 of thesubjects exceeded a change of 0.05 m/s after the 12-session
These results provide preliminary support for the use of WBV as
intervention of WBV. Subject 13 was unable to take a single step in
an intervention to improve walking function in individuals with
the initial test. After the 12-session intervention of WBV, the
SCI, with changes that appear to be comparable to those achieved
subject was able to take four steps. It could be argued that this
with some forms of locomotor training. With a 12-session
magnitude of change may be even more meaningful in individuals
intervention of WBV, we found significant improvements in
with SCI than it is in healthy elders. Our findings are consistent
walking speed, cadence, step lengths, and intralimb coordination
with improvements in walking function observed in elderly
over multiple steps. Furthermore, the effect of WBV on walking
individuals and in individuals with Parkinson's disease who
function may continue to improve walking function even after the
received a WBV intervention and therefore provide pre-
use of WBV has ended. However, this was assessed in a single
liminary evidence that regular use of WBV may be a potent
subject and requires further investigation.
intervention for improving walking function in individuals withSCI.
In the single subject who performed a follow-up test session 5
Conflict of interest
weeks after the WBV intervention, the effects on walking speed notonly persisted, but increased 5 weeks after the WBV intervention.
There is no conflict of interest with any of the authors.
These are similar to findings in individuals with Parkinson'sdisease who had a persistent change in walking speed 4 weeks
after receiving a 3-week WBV intervention . The use of afferentinput to induce positive plastic effects in the nervous system has
We gratefully acknowledge the technical contributions of
received considerable attention in the recent research literature
Stephen Lindley. This study was supported by The Miami Project
These plastic changes are most meaningful when they are
to Cure Paralysis and the NIH grant #R01HD41487.
associated with a lasting improvement in function . Futurestudies should assess the persistence of effects of WBV through
follow-up testing performed some time after the final intervention.
We observed improvements in cadence, step length of the
[1] Ditunno PL, Patrick M, Stineman M, Ditunno JF. Who wants to walk? Prefer-
strong and weak legs, and consistency of hip-knee intralimb
ences for recovery after SCI: a longitudinal and cross-sectional study. SpinalCord 2008;46(7):500–6.
coordination after a 12-session intervention of WBV. Furthermore,
[2] Perry J. Pathological mechanisms. In: Gait Analysis Normal and Pathological
changes in walking speed and cadence were moderately correlated
Function; 1992. p. 169–182.
suggesting the increase in walking speed associated with the WBV
[3] Krawetz P, Nance P. Gait analysis of spinal cord injured subjects: effects of
injury level and spasticity. Arch Phys Med Rehabil 1996;77(7):635–8.
intervention is related to an increase in the number of steps taken
[4] Stein RB, Chong S, James KBCJWM. Devices for improved mobility after spinal
per minute. In addition to an increase in cadence, changes in
cord injury and stroke. In: Proceedings of the 20th annual international
walking speed also had a fair relationship with changes in the
conference of the IEEE engineering in Medicine and Biology Society, vol.
20; 1998. p. 2297–300.
stronger step length, suggesting that increased stronger leg step
[5] Ivanenko YP, Grasso R, Lacquaniti F. Influence of leg muscle vibration on
lengths may also contributed to the improvements in walking
human walking. J Neurophysiol 2000;84(4):1737–47.
Please cite this article in press as: Ness LL, Field-Fote EC. Whole-body vibration improves walking function in individuals with spinalcord injury: A pilot study. Gait Posture (2009),
G ModelGAIPOS-2815; No of Pages 5
L.L. Ness, E.C. Field-Fote / Gait & Posture xxx (2009) xxx–xxx
[6] Novak P, Novak V. Effect of step-synchronized vibration stimulation of soles on
[18] Scivoletto G, Romanelli A, Mariotti A, Marinucci D, Tamburella F, Mammone A,
gait in Parkinson's disease: a pilot study. J Neuroeng Rehabil 2006;3:9.
et al. Clinical factors that affect walking level and performance in chronic
[7] Gurfinkel VS, Levik YS, Kazennikov OV, Selionov VA. Locomotor-like move-
spinal cord lesion patients. Spine 2008;33(3):259–64.
ments evoked by leg muscle vibration in humans. Eur J Neurosci 1998;10(5):
[19] Field-Fote EC, Tepavac D. Improved intralimb coordination in people with
incomplete spinal cord injury following training with body weight support
[8] Kawanabe K, Kawashima A, Sashimoto I, Takeda T, Sato Y, Iwamoto J. Effect of
and electrical stimulation. Phys Ther 2002;82(7):707–15.
whole-body vibration exercise and muscle strengthening, balance, and walk-
[20] Nash MS, Meltzer NM, Martins SC, Burns PA, Lindley SD, Field-Fote EC.
ing exercises on walking ability in the elderly. Keio J Med 2007;56(1):28–33.
Nutrient supplementation post ambulation in persons with incomplete spinal
[9] Roelants M, Delecluse C, Verschueren SM. Whole-body-vibration training
cord injuries: a randomized, double-blinded, placebo-controlled case series.
increases knee-extension strength and speed of movement in older women.
Arch Phys Med Rehabil 2007;88(2):228–33.
J Am Geriatr Soc 2004;52(6):901–8.
[21] Dobkin BH. Progressive staging of pilot studies to improve phase III trials for
[10] Ahlborg L, Andersson C, Julin P. Whole-body vibration training compared with
motor interventions. Neurorehabil Neural Repair 2009;23(3):197–206.
resistance training: effect on spasticity, muscle strength and motor perfor-
[22] Marino RJ, Barros T, Biering-Sorensen F, Burns SP, Donovan WH, Graves DE,
mance in adults with cerebral palsy. J Rehabil Med 2006;38(5):302–8.
et al. International standards for neurological classification of spinal cord
[11] Ebersbach G, Edler D, Kaufhold O, Wissel J. Whole body vibration versus
injury. J Spinal Cord Med 2003;26(Suppl 1):S50–6.
conventional physiotherapy to improve balance and gait in Parkinson's dis-
[23] Tepavac D, Field-Fote EC. Vector coding: a technique for quantification of
ease. Arch Phys Med Rehabil 2008;89(3):399–403.
intersegemental coupling in multicycle behaviors. J Appl Biomech 2001;17:
[12] Gianutsos J, Oakes LC, Siasoco V, Appelblatt S, Hamel J, Gold J. Motor reha-
bilitation of spinal cord dysfunction by means of whole body vibration. In:
[24] Portney LG, Watkins MP. Correlation. In: Foundations of clinical research; 3rd
Abstract presented at 3rd mediterranean congress of physical medicine and
[25] Perera S, Mody SH, Woodman RC, Studenski SA. Meaningful change and
[13] van Nes I, Geurts AC, Hendricks HT, Duysens J. Short-term effects of whole-
responsiveness in common physical performance measures in older adults.
body vibration on postural control in unilateral chronic stroke patients:
J Am Geriatr Soc 2006;54(5):743–9.
preliminary evidence. Am J Phys Med Rehabil 2004;83(11):867–73.
[26] Conforto AB, Kaelin-Lang A, Cohen LG. Increase in hand muscle strength of
[14] van Nes I, Latour H, Schils F, Meijer R, van KA, Geurts AC. Long-term effects of
stroke patients after somatosensory stimulation. Ann Neurol 2002;51(1):122–
6-week whole-body vibration on balance recovery and activities of daily living
in the postacute phase of stroke: a randomized, controlled trial. Stroke
[27] Hoffman LR, Field-Fote EC. Cortical reorganization following bimanual train-
ing and somatosensory stimulation in cervical spinal cord injury: a case report.
[15] Ness LL, Field-Fote EC. Effects of whole body vibration on spinal reflex activity
Phys Ther 2007;87(2):208–23.
and walking function in individuals with chronic, motor incomplete spinal
[28] Rosenkranz K, Rothwell JC. Differences between the effects of three plasticity
cord injury. In: Neuroscience 2008; 2008.
inducing protocols on the organization of the human motor cortex. Eur J
[16] Field-Fote EC, Lindley SD, Sherman AL. Locomotor training approaches for
individuals with spinal cord injury: a preliminary report of walking-related
[29] Verschueren SM, Swinnen SP, Desloovere K, Duysens J. Effects of tendon
outcomes. J Neurol Phys Ther 2005;29(3):127–37.
vibration on the spatiotemporal characteristics of human locomotion. Exp
[17] Lapointe R, Lajoie Y, Serresse O, Barbeau H. Functional community ambulation
Brain Res 2002;143(2):231–9.
requirements in incomplete spinal cord injured subjects. Spinal Cord
[30] Courtine G, Pozzo T, Lucas B, Schieppati M. Continuous, bilateral Achilles' tendon
vibration is not detrimental to human walk. Brain Res Bull 2001;55(1):107–15.
Please cite this article in press as: Ness LL, Field-Fote EC. Whole-body vibration improves walking function in individuals with spinalcord injury: A pilot study. Gait Posture (2009), doi:
Source: http://www.power-plate.fr/files/whole-body-vibration-improves-walking-function-in-individuals-with-spinal-cord-injury-a-pilot-study-oWjrXya.pdf
Published May 3, 1999 Inhibition of T Cell Proliferation by MacrophageTryptophan Catabolism By David H. Munn,*‡ Ebrahim Shafizadeh,* John T. Attwood,*Igor Bondarev,* Achal Pashine,* and Andrew L. Mellor* From the *Institute of Molecular Medicine and Genetics and the ‡Department of Pediatrics, Medical College of Georgia, Augusta, Georgia 30912
Annual Report for the year ending 31st December 2009 Investing in your FutureSupporting the Creation & Development of Local Enterprise Mike Cantwell Asst. CEO & Mairead Barron St. Joseph's Sean Gallagher, Ned Toomey CEO & Secondary School Doon, Co. Limerick Agnes Relihan Business Advisor New Horizons Networking Event with Mid