Www-scf.usc.edu
Republic of Kenya
MINISTRY OF HEALTH
CONTROL OF JIGGER
DIVISION OF ENVIRONMENTAL HEALTH
1 National Policy
Guidelines on Prevention
and Control of Jigger

AcknowledgementThe development of this policy guideline for jigger prevention and control in Kenya has been made possible through the concerted efforts of many organizations and individuals. The document went through different developmental stages and reviews.
The Ministry of Health would like to extend appreciation to all individuals and teams who participated in the process of developing the policy guidelines. We acknowledge the special contribution of Dr. John Kariuki, Deputy Director, Public Health; P. Wanjohi, Vector and Vermin Control Section, Division of Environmental Health; Dr. Lynne Elson, Malindi Jigger Working Group/Malindi Public Health Office; Christine W. Banga, Catholic Relief, Kenya; John Collett, EARO/World Vision; and James Kiptoon, Samburu County Vector and Vermin Control focal-person, all of whom took leading roles in the process of developing this document.
Special thanks also go to Mr. Tobias Omufwoko, Kenya WASH Alliance; Evelyn Makena, WASHPLUS- Family Health International (FHI360) and Wanjiku Kuria, World Vision, Kenya for financing and moderating the development of these policy guidelines.
We also single out the invaluable contribution and inputs from John Mwasaru, SPHO ,Taita Taveta county; Charles Ngira, PLAN KENYA; Vincent Iduri, CPHO Kilifi; Bernard N.Mureka, CPHO Bungoma; John G. Mugenyo,CPHO Nyeri;Christopher Nzioka,KWAHO;Harun Ngotho, SACPHO, Nairobi County; Alfred Muli,Wash United; Benjamin Murkomen ,DEH-MOH; Janet Mule, DEH_MOH; Sharon Lipesa, WASH hub, DEH-MOH; Arnold Wafula, WASH hub, DEH-MOH; Neville Okwaro, WASH hub, DEH –MOH; Hillary Okumu ,SPHO, Siaya county; Paul N. Kamau, CPHO Murang'a County; Farida Tomno, MOH- HPU; Jemmimah W. Kamau, SPHO, Kericho County; Lucy M. Goro, Living Water S,C; Tabitha Gerrets, MWA; Denis Munai, Kenya Wash Alliance; Senan Kanana, MWA; Dr. Tatu Kamau,MOH- VBDU; Wyckliff Omondi, MOH- NTDU; Lenson Kariuki, MOH-VBDU; Emmanuel Luvai, SPHO, Busia County; Judith A. Anyango, SPHO, Kisii County; Susan Karanja; Ahadi Kenya Trust; Cate Mayeye; Ahadi Kenya Trust ;Joy Melly,Fhi360;Grace Wasike, MoH- Child Health; Mika Mitoko, Path; and Mr.Ngaruia, MOEST-Basic Education.
The Ministry of Health further acknowledges the technical advice and contribution made by Prof. M. Karama, Kenya Medical Research Institute (KEMRI); and the useful insights given by Dr. Stanley Kamau, Ahadi Kenya Trust.
Kepha Ombacho, PhD, MBS
Director, Public Health
Ministry of Health
Guidelines on Prevention
and Control of Jigger

ForewordJigger infestation is one of the neglected public health problems in Kenya affecting over 4% of the population especially among the poorest households in endemic and high transmission counties. Its complications are a leading cause of disability, morbidity and sometimes mortality, particularly in school age children, the elderly, and people living with physical and mental disabilities. Per capita social economic losses attributable to the disease have not been computed, but according to S.K. Ruttoh and others who studied the problem in 2010, these are considerable .The school hours lost by infested children due to inability to walk, decreased agricultural productivity of infested adults and loss of social capital due to stigma associated with the disease all hampers wholesome participation in nation-building by both the infested and the affected. As such, jigger infestations frustrates Kenya's attempts to achieve the Millennium Development Goal on poverty reduction by the year 2015 as well as reducing the pace of national development envisioned in Kenya's Vision 2030.
Therefore, for the country to achieve Vision 2030 and Millennium Development Goals, there is an urgent need to contain the disease once and for all. The Ministry of Health has prioritized this objective, with the Division of Environmental Health (DEH) coordinating the effort. The DEH promotes the implementation of technically sound jigger prevention and control interventions. One of such interventions is regular fumigation of infested households, on-host treatment of reservoir animals, hygiene promotion and education as well as disinfection of jigger wounds to prevention complications including secondary infections, disability and death.
It should be noted that Tungiasis, which is the illness arising out of infestation of man by Tunga penetrans has no effective curative treatment. Only effective vector control has potential for massive reduction of the jigger infestation burden and eventual elimination of jiggers in the country. However this intervention is expensive and involves heavy financial outlay for procurement of commodities and other logistics of application. It is therefore necessary and prudent for the Ministry and public health departments to engage with various stakeholders and partners if quick gains are to be realized. Application of the public health mantra of "prevention is better than cure" is also necessary through promotion of environmental and personal hygiene for the prevention of jigger breeding and infestation. Strategic Plans need to be formulated in line with these guidelines to guide implementation of scientifically sound jigger prevention and control interventions that aim to eliminate jiggers in small bits, probably village by village or county by county, with transparent monitoring and evaluation mechanisms, until the whole country is declared free of jiggers.
Finally, I would like to recommend this policy guideline to all partners and stakeholders in the country. It provides useful information on how to prevent, control and eventually eliminate jiggers in the country using the most effective, efficient and affordable methods. It emphasizes the usefulness of surveillance, prevention, control, monitoring and evaluation to guide project and programmatic operational plans.
I hope the users of this document will find it useful in achieving our vision of a jigger-free Kenya.
James W. Macharia
Cabinet Secretary
Ministry of Health
3 National Policy
Guidelines on Prevention
and Control of Jigger

Abbreviations and Acronyms
Division of Environmental Health
Pest Control Products Board
Kenya Bureau of Standards
National Environmental Management Authority
Kenya Medical Research Institute
Vector Borne Diseases Unit
World Health Organization
Human Immunodeficiency Virus
County Government(s)
Information Education and Communication
Out Patient Department
Centers for Disease Control
Ministry of Health
Guidelines on Prevention
and Control of Jigger

1.0. Introduction
Life Cycle of a Jigger Flea (courtesy of CDC)
Pathology (Fortaleza Process)
Aim of the Guidelines
Objectives of the Guidelines
Justification for the Guidelines
Guidelines on Jigger Prevention and Control Strategies
Institutional Roles
Ministry of Health (MOH)
Ministry of Agriculture Livestock Development and Fisheries
Ministry of Education Science and Technology 13
Ministry of Environment Water and Natural Resources 13
Ministry of Interior Coordination
Departments of Health
Department of Education
Health Departments 14
Private and non-governmental Sector
Community-Based Organizations
2.11. Households
Recommended Jigger Prevention and Control Measures
Environmental and Personal Hygiene
Traditional (Primordial) Methods
Biological Control
Mechanical or Physical Control
Chemical Control
Guide for Regulation of Vector and Vermin Control Operators
Guidelines for Equipment and Chemicals
Guidelines for Licensing of Vector and Vermin Control Operators
Health and Safety Considerations in Pesticide Use
Tungiasis Treatment and Care
9.0. Conclusions
Policy Recommendations
11.0. References
12.0. Annexures
Annex A: Model Regulations for Pest Control Operators
Annex B: Recommended Criteria for Licensing Private Sector Participants
Annex C: List of Common Chemicals for Use in Domestic Pest and Vector Control that can
also be Used to Control Jigger Infestations
Annex D: Jiggers (Tungiasis) Notification and Investigation Form
Annex E: Community Health Extension Worker Summary on Jiggers
5 National Policy
Guidelines on Prevention
and Control of Jigger

1.0. Introduction
Jiggers (Tungiasis) is an important but neglected public health problem in Kenya. It is a vector-borne disease caused by the Jigger flea, also known as sand flea, Funza, Ndutu, Dudu, Chigoe or Tunga penetrans, an ecto-parasite which causes Tungiasis. It is a parasitic condition of humans and animals. Tetanus is a common secondary infection that has been associated with deaths of jigger victims and the spread of HIV/AIDS which is passed from one person to person due to sharing of pins. The flea affects many impoverished communities and families in the country. An estimated 1.4 million Kenyans translating to 4 percent of the total population suffer from jigger infestation, with the highest prevalence rates found in Central, Nyanza, Western, Coast and Rift valley regions. These are Baringo, Bomet, Bungoma, Busia, Elgeyo Marakwet, Homa Bay, Kakamega, Kericho, Kiambu, Kilifi, Kirinyaga, Kisii, Kwale, Marsabit, Migori, Murang'a, Nandi, Nyamira, Nyeri, Samburu, Siaya, Taita-Taveta, Uasin Gishu and Vihiga counties. The most at risk population cohorts are children 5 to 14 years, the elderly, and the physically and mentally disabled persons in the affected areas, that is, approximately 10 million Kenyans (MOH, 2013). The severity of jigger infestation is its generalization in the affected parts i.e. in the foot, fingers, knees, elbows thus causing serious difficulty in walking and reducing the infected person's ability to work normally and look for income to feed their families or attend school. In endemic areas, prevalence ranges from 15-40% of the population1.
Epidemiologically, person to person transmission is not possible. The jigger must go through phases of its life cycle in sandy, dusty soil before becoming infective to another human. Animals can also be infected with jiggers and serve as reservoir hosts continuing the cycle and contamination of the environment. These include a broad spectrum of animals, with chickens, pigs, dogs, cats and rats as the principal reservoirs in resource poor settings. Poor hygiene habits such as infrequent bathing and feet washing increase the chances of a person becoming infested.
Household poverty has been linked to the health conditions of the occupants since it determines the family's ability to access good quality housing, clean water, sanitation and good nutrition. Thus jigger infestation tends to be linked to poverty, poor community participation in hygiene and sanitation education, Negative health seeking behavior and indiscriminate waste disposal methods in the villages.
On the social economic front, Jigger infestations lead to many affected children dropping out of school as they are unable to walk to school and also because they face the challenge of stigmatization and discrimination. This leads to a vicious cycle of poverty, ignorance and disease. The other determinants of jigger infestations are age (the early childhood and elderly cohorts are disproportionately affected) and physical and mental disabilities. If the country is to deal effectively with the jigger menace, health, developmental and humanitarian actors in government, civil society and community need to understand prevailing practices, perceptions, attitudes and knowledge gaps that lead to the problem. They need also to understand the environmental and socio-economic risk factors that can be curtailed to control, prevent or eradicate jigger infestations. This
Guidelines on Prevention
and Control of Jigger
guideline provides information on the current practices available for the control of jiggers to be used as a resource for the many players to decide on the best way forward in their circumstances. The ultimate strategy is to use a combination of interventions targeting the infected people, reservoir animals and the environment.
The first recorded mention of this parasitic infection was by Gonzalez Fenadez who, in 1525 described many instances of Spanish conquerors in Haiti who suffered from it. It is thought that jiggers were brought to East Africa by migrants from India who constructed the railway from Mombasa to Kampala in the 19th century. Others say they came to Africa aboard a British ship that sailed from South America to West Africa, and then spread inland towards the east of the continent. Over time locals were severely infested. One observer near the turn of the last century called jiggers "the most fearful calamity that has ever afflicted the East African peoples" after seeing affected people on the slopes of Mount Kilimanjaro crawling around on all fours and groaning with pain. Inadequate water supply and poor hygiene are blamed for the infestation. However, some affected people think they are bewitched and simply let them run their course instead of trying to remove the insects.
Tunga penetrans is a parasitic arthropod found in most tropical and sub-tropical climates. Its head is angular, it has no comb of spines, and the thoracic segments are narrow at the top. Tungiasis is the condition caused by female T. penetrans when it embeds in human skin.
Males leave the host after a blood meal like other fleas, but the female flea burrows head-first into the host's skin, leaving the caudal tip of its abdomen visible through an orifice in a skin lesion. This orifice allows the flea to breathe, mate, defecate and reproduce while feeding on blood vessels in the cutaneous and subcutaneous dermal layer. Over the next two weeks, its abdomen swells, in a process called neosomy, with up to several dozen eggs, which it then releases through the caudal orifice to fall to the ground when ready to hatch. The flea then dies and is sloughed off with the host's skin. Within the next three to four days, the eggs hatch, and mature into adult fleas within three to four weeks. On burrowing and feeding on blood inside the skin of its host, the female's abdomen becomes enormously enlarged between the second and the third segments so that the flea forms a round sac with the shape and size of a pea. Tunga penetrans predilection sites in the skin are under the toenails and fingernails of man-where the resultant sores may fill with pus and become infected.
The first evidence of the infestation by this sand flea is a tiny black dot on the skin at the point of penetration. Because the flea is a poor jumper, most lesions occur on the feet, often on the soles, the toe webs and around or under the toenails. A small inflammatory papule with central black dot forms early. Within the next few weeks, the papule slowly enlarges into a white, pea-sized nodule with well defined borders between 4-10mm in diameter. This lesion can range from asymptomatic to pruritic to extremely painful. Multiple/severe infestations may result in a cluster of nodules with a honey comb appearance.
7 National Policy
Guidelines on Prevention
and Control of Jigger
Medically, tungiasis is considered an entomologic nuisance and does not receive much attention. It is a problem that is debilitating to those affected, but which the medical profession and the scientific community neglect.
In Kenya, jigger prevention and control have been prioritized by the ministry of health under the Division of Environmental health. The main approaches have been treatment, hygiene promotion, chemical control and community strategy. Treatment has been done at facility and outreach camps by soaking infested feet in antiseptic solution mainly potassium permanganate and hydrogen peroxide. According to the Clinical Guidelines for Diagnosis and Treatment of Common Conditions in Kenya (MOH 2002), extraction of the jiggers with clean pin is advocated as well as suffocation of jiggers by soaking feet in Liquid paraffin or Kerosene and administration of Tetanus Toxoid. However, these treatment regimes are of no proven efficacy2.
Prevention and control has been through hygiene education and use of insecticidal sprays and dusts on infested households and schools. But these are high cost interventions and the activities are not well funded.
In the last ten years, civil society organizations and NGOs have also come out strongly to support the ministry in awareness creation, advocacy, treatment and control. However, while their efforts and those of the government have brought some relief on affected patients and households, they have not even begun to impact on the country's big jigger infestation burden.
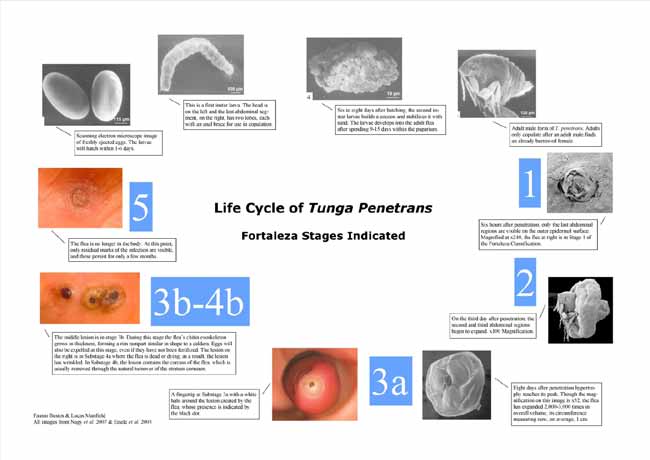
1.2. Life Cycle of a Jigger Flea
Guidelines on Prevention
and Control of Jigger
As illustrated in the life cycle figure from the previous page, the eggs, larvae and pupae live in the soil. It is only the adult female that burrows into the skin of humans and animals. Tungiasis is almost invariably associated with an intense inflammation around embedded fleas, and is associated with considerable morbidity.
Super-infection of the lesions is virtually constant, and a variety of aerobic and anaerobic bacteria have been isolated from embedded sand fleas. Fissures, severe inflammation, fibrosis, sepsis, ulcers, gangrene, localized edema, lymphedema, deformation and loss of nails and auto-amputation of digits are known sequels. In non-immune individuals, tungiasis is a risk factor for tetanus.
An infestation begins to irritate and itch when the female is almost fully developed.
Sometimes it causes severe inflammation and ulceration. When the female flea dies in the skin it may cause a secondary infection which, if ignored, could lead to tetanus, gangrene and even the loss of a toe.
Natural extrusion of the egg sac or removal of the jigger with a dirty pin or needle leaves a tiny pit in the skin which may develop into a sore in which pus forms. The sore may extend and develop into a septic ulcer. An infection under a toenail may cause the nail to be lost.
1.4. Clinical pathology (Fortaleza Process)
As parasites tend to accumulate at certain predilection sites, the pathologic findings should be particularly severe in these sites. Many infected persons have lesions in the periungual region of the toes, which explains the high frequency (69%) of nail deformation or nail loss in jigger victims. Furthermore, as the sole of the feet and the heel are other predilection sites, difficulty in walking is also very common.
Various mechanisms exist by which embedded fleas could induce pathologic alterations of the skin in an early stage of development. Acute inflammation with erythema, edema, pain, and itching is conceivably due to tissue damage induced by a metabolically highly active and continuously enlarging parasite. As with other blood-sucking insects, T. penetrans releases proteolytic enzymes during penetration and growth, causing an inflammatory response of the skin. In comparison with other ectoparasites that frequently re-infect humans, the immune response of the host might contribute to the intense inflammation observed soon after penetration.
As the lesion develops, bacterial super-infection almost inevitably occurs. During penetration, the flea breaks up the stratum corneum, allowing bacterial micro colonies on the skin surface to spread. In addition, pathogenic microorganisms on the outer surface of the flea may be actively carried into the epidermis. As the continuously expanding body of the flea (the volume increases by a factor of roughly 2,000) consists of rather smooth intersegment skin and newly formed chitinous clasps, the embedded flea fulfills the requirement of a structural matrix to which microorganisms could easily
9 National Policy
Guidelines on Prevention
and Control of Jigger
adhere. In fact, scanning-electron microscopy of extracted fleas showed that pathogens such as streptococci and gram-negative rods formed a biofilm in the tiny grooves of newly built intersegment skin as well as on the chitinous exoskeleton of the parasite.
As the lesion itches immediately after the flea penetrates, patients usually start to scratch, which, in turn, promotes the entry of bacteria through the persistent sore in the epidermis. In fact, micro abscesses can be observed in histological sections of lesions only 2 days after penetration.
In many patients, bacterial super-infection is also the result of an inappropriate manipulation of lesions with non-sterile instruments by the patient or caregiver. The remarkable desquamation of the skin observed around late-stage lesions has its histopathology correlates in hyperkeratosis and parakeratosis of the stratum corneum.
Reports on severe tungiasis involve persons with particular risk factors, such as alcoholics or the mentally diseased, who are expected to have prolonged contact with the ground or are unable to care for themselves. Data also show that severe tungiasis also occurs in persons without such risk factors who live in an impoverished household, where environmental, socioeconomic, and behavioral factors coexist and make frequent re-infection likely or impede the extraction of penetrated fleas in the early stage. Estimates show that 10 million Kenyans who live in households with such environmental and social-economic characteristics are at risk of tungiasis.
Guidelines on Prevention
and Control of Jigger
Although there are no accurate figures, the estimated 4% of severe tungiasis in the general population means that at least the same proportion of patients arriving at the OPDs for reasons unrelated to the ectoparasitosis have tungiasis as well. It is important therefore for clinicians to watch out for the main tungiasis sequilae and treat accordingly.
Thus, clinicians should independently diagnose tungiasis during consultation through physical inspection of predilection sites of susceptible patients especially children, the elderly and the physically or mentally handicapped whether or not the condition is mentioned by the patient.
But poverty, social neglect, and inadequate health seeking behavior among jigger patients imply that the bulk of tungiasis diagnosis can only be done at the community or household level through community health extension.
There are no diagnostic tests for tungiasis. This is most likely because the parasite is ectoparasitic with visible symptoms.
Beside humans, T. penetrans parasitizes a range of domestic animals, such as dogs, cats, chicken, pigs and rodents. Dogs and cats act as important reservoirs for the intra- and peri-domiciliary transmission of sand fleas. When humans live in close contact with infested animals, the risk of infestation is high and the intensity of infestation is high.
T.penetrans exists in all tropical areas of the world including Latin America, the Caribbean, and sub-Saharan Africa. The majority of those infested are children (75%), the elderly, the mentally and physically disabled and alcoholics. The latter adult groups likely because they spend long periods of time in one place with their feet on the soil and may have sub-optimal immune responses. Heavy infestations are also associated with poverty since impoverished families lack closed shoes, sealed house floors, soap, water, education and good nutrition.
Seasonal variations of tungiasis have been observed. Disease occurrence decreases as soon as the rainy season starts and re-increases with the beginning of the dry season. Therefore high-impact interventions such as spraying should be done at the beginning of the dry seasons4.
1.5. Aim of the Guidelines
To guide the control and eventual elimination of jigger infestations in the country.
1.6. Objectives of the Guidelines
1. To strengthen capacity for jigger prevention and control at the county and national
levels of government.
2. To guide the use of pesticides for control of jiggers in infested households, schools
and other institutions.
11 National Policy
Guidelines on Prevention
and Control of Jigger
3. To promote sustainable jigger prevention and control mechanisms at the
community level.
4. To guide the activities of various actors in jigger prevention, treatment and control.
5. To guide health workers on treatment of jigger – infested patients.
6. To advocate for surveillance mechanisms for jigger prevalence and evaluation of
jigger control programs.
7. To stimulate research on various aspects of jigger prevention and control
1.7. Justification for the Guidelines
Jiggers (Tungiasis) afflicts 4% of the population in Kenya. Another 25%, mainly children, are at risk of infestation. They contribute to significant morbidity and sometimes mortality in endemic counties.
Lack of standardized approaches to prevention, control and treatment and the widespread use of harmful or ineffective approaches can be attributed to the lack of national guidelines and awareness.
1.8. Guidelines on Jigger Prevention and Control Strategies
Jigger prevention and control programs and projects should endeavor to:1. develop strategic plans with clear objectives, outputs and outcomes for sustainable
jigger prevention and control activities in line with the National Development agenda and Millennium Development Goals.
2. foster collaboration among key Stakeholders (Ministries and Departments of
Health, Education, Science, Water, Agriculture and Academic and Research Institutions, Industries, communities, organizations, victims etc,) on issues of jigger prevention, control and eventual elimination.
3. support research into environmentally friendly methods of jigger control.
4. sensitize and mobilize communities on the significance of personal hygiene and
other environmentally friendly jigger prevention methods.
5. facilitate the establishment/strengthening of jigger prevention and control
programs, projects and activities in relevant ministries, departments, agencies at county and national governments.
6. foster private and non-governmental sector participation in jigger prevention and
7. conduct a comprehensive baseline survey of jigger infested people and households
and their characteristics.
8. develop user friendly prevention, control and treatment manuals for use by health
practitioners and other actors.
9. identify areas mostly affected in terms of vulnerability to jiggers.
10. set up sustainable measures towards ensuring good hygienic practices and
behavior change. This includes long term WASH interventions, housing improvement and poverty alleviation.
Guidelines on Prevention
and Control of Jigger

2.0. Institutional Roles
2.1. Ministry of Health (MOH)
1. Develop prevention, control and treatment guides for use by health practitioners
and humanitarian actors.
2. Provide technical assistance and logistic support to counties on jigger prevention
and control.
3. Develop Information, Education and Communication (IEC) materials for jigger
prevention and control in consultation with county health departments and other stakeholders.
4. Build capacity and ensure institutional strengthening for jigger prevention and
5. Conduct in collaboration with relevant stakeholders, mass jigger treatment camps
in endemic areas for hard-to-reach infested people.
6. Encourage private and non-governmental sector participation in jigger prevention
and control services.
7. Conduct quarterly Monitoring and Evaluation of jigger prevention and control
8. Collaborate with relevant Ministries (Agriculture, Health, Science and Technology
and Education etc.) on research into better methods of jigger prevention and control.
2.2. Ministry of Agriculture Livestock Development and Fisheries
1. Develop better farming and animal husbandry techniques for poverty alleviation in
affected rural households.
2. Collaborate with Ministry of Health in the continuous review and registration of
appropriate pesticides for the control of jiggers through the Pest Control Products Board (PCPB).
2.3. Ministry of Education Science and Technology
1. Collaborate with the Ministry of Health to undertake research, foster the
development and dissemination of new and better methods of jigger prevention and control.
2. Collaborate with Ministry of Health to conduct treatment of school compounds
and students.
3. Develop jigger prevention and control curriculum for learners.
2.4. Ministry of Environment Water and Natural Resources
1. Facilitate the provision of subsidized portable water for infested households.
2. Approve and monitor chemical control of jigger infestations in schools and households.
13 National Policy
Guidelines on Prevention
and Control of Jigger
2.5. Ministry of Interior and Coordination of National Government
1. Facilitate household surveys for the purposes of identifying jigger infested
households and individuals in the community.
2. Facilitate the registration and operations of NGOs, CBOs and community support
groups for jigger infested members of the community.
3. Encourage infested individuals to seek medical attention.
4. Facilitate the work of health extension workers in the community.
5. To participate in planning, community mobilization and implementation of jigger
treatment medical camps and awareness creation events.
6. Uphold the rights of jigger infested households and individuals to healthcare and
social support.
2.6. County Departments of Health
1. Implement these Policy Guidelines at the county level.
2. Generate data on jigger prevention and control activities in their counties.
3. Supervise and coordinate jigger prevention and control programs at the County
Government level.
4. Provide technical support to NGOs involved in jigger prevention and control
5. Carry out advocacy at the county level.
6. Conduct periodic monitoring and evaluation at the County Government levels.
7. Adapt in collaboration with stakeholders, jigger prevention and control plans of
action for the counties.
8. Build capacity of jigger prevention and control personnel.
9. Sensitize and mobilize communities using Information, Education and
Communication (lEC) materials.
10. Encourage private sector participation in jigger prevention and control services11. Prepare quarterly reports on jigger prevention and control activities and send to the
national Ministry of Health.
2.7. County Department of Education
1. Collaborate with County departments of health and other relevant stakeholders in
dissemination of IEC materials to the communities.
2. Support national Ministry of Health in generating data on jigger prevention and
control activities in their counties.
3. Collaborate with Ministry of Health and county department of health to conduct
treatment of school compounds and students.
4. Advise schools on formation of jigger prevention control health (hygiene) clubs.
2.8. Sub-county Health Departments
1. Develop a comprehensive line list of jigger-infested individuals and map out affected
households and schools.
2. Implement routine jigger prevention and control activities in the communities.
Guidelines on Prevention
and Control of Jigger
3. Ensure private sector participation in jigger prevention and control activities.
4. Sensitize and mobilize communities using lEC materials.
5. Make annual budget for jigger prevention and control activities for onward
transmission to county health departments.
6. Monitor the activities of non-governmental organizations doing jigger prevention and
control activities to ensure compliance with the guidelines and codes of practice.
7. Supervise and coordinate jigger prevention and control activities at community level.
8. Render monthly reports on jigger prevention and control activities and forward to
2.9. Private and non-governmental Sector
1. Comply with the provisions of the National Policy Guidelines on jigger prevention
and control.
2. Participate in jigger prevention and control services on humanitarian basis.
3. Engage in partnership with county and national Governments for better service
4. Undertake and support research, specialized studies and product development in
jigger prevention and control.
5. Promote public awareness campaigns.
2.10. Community-Based Organizations
1. Undertake grassroots mobilization to participate in jigger prevention and control.
2. Promote jigger prevention and control at household level.
3. Promote public awareness campaigns on appropriate strategies for jigger
prevention and control.
1. Adopt anti-jigger habits and practices.
2. Comply with existing laws and regulations on jigger prevention and control.
3. Comply with the provisions of these Policy Guidelines.
4. Cooperate with other stakeholders to ensure sustainable jigger prevention and
5. Present themselves for jigger treatment at health facilities and attend mass
treatment camps.
15 National Policy
Guidelines on Prevention
and Control of Jigger
3.0. Recommended Jigger Prevention and
Off-host stages of T. penetrans develop best in dry soil or in dusty soil containing organic material. Measures aiming to interrupt the off-host development should therefore focus on physically changing the environment in which eggs, pupae, and larva develop.
This can be done through paving streets, cementing floors, and eliminating uncontrolled disposal of waste in public areas and private compounds. However, these interventions require substantial funds and are beyond the economic capabilities of most communities where tungiasis is endemic.
However, there are some jigger prevention and control measures that are doable at the household and community levels. These include:
3.1. Environmental and Personal Hygiene
• Suppressing dust by wetting the house and compound floors after thorough
sweeping away of food remains, litter and other debris.
• Environmental cleanliness is very effective for controlling jiggers and other vectors
and can lead to elimination, which can be sustained through health education and community sensitization.
• Keeping nails short by clipping. • Daily feet washing and regular bathing with soap and water. • Constant wearing of closed shoes.
• The elimination of breeding sites or hide outs for jiggers include general cleaning of
house floors, compounds, etc.
• Removing sources of food for rats or mice e.g. prompt clean up after cooking and,
regular garbage disposal, and rat-proofing of dwelling houses and granaries etc.
• Removal of domestic jigger reservoir animals including dogs, cats, goats, pigs, sheep
and chicken from dwelling houses.
3.2. Traditional (Primordial) Methods
Time-tested and effective cultural and traditional methods of household vector and vermin control e.g. the use of materials like slime mixed in ash to regularly smear floors and walls of dwelling houses built in temporary materials removes breeding places or repels jigger fleas. The traditional method of dust-suppression by regular wetting of dusty floors is also a domestic hygiene practice in traditional communities.
3.3. Biological Control
1. The use of natural methods to control jiggers such as certain plant extracts. 2. The use of plant extracts as repellants e.g. neem, aloe vera and coconut oil as
topical applications has been shown to be effective and environmentally friendly
Guidelines on Prevention
and Control of Jigger
jigger repellents which also induce considerable remission in clinical pathology. These can be provided to victims and those at risk for regular use.
3. Treatment of house floors and outdoor resting areas with neem solution which is
environmentally friendly and non-toxic.
3.4. Mechanical or Physical Control
The use of devices, machines, barriers and other mechanized methods to control jiggers or alter their environment e.g. shoes, and the plastering of floors with cement mortar, and the regular cleaning of these floors with water are known to reduce jigger flea infestations in the environment to negligible levels.
These long-term, safe and environment friendly methods are effective as long as the devices are intact, and the floors and walls are not dusty or chipped. But they imply the need for considerable social economic support for jigger-infested households, most of whom are very poor or deprived.
3.5. Chemical Control
The use of chemicals to destroy jiggers, control their activity or prevent them from causing damage is very effective.
Pesticides either kill or repel the jiggers and are therefore, the fastest ways to control them. The use of non-persistent and other environment friendly chemicals is recommended. These include ICON or hypercypermethrin spray, Carbaryl insecticidal dust, Propoxur insecticidal dust or spray, Deet topical repellant, e.t.cThe use of Carbaryl dust on infested homestead floors has a particularly strong knockdown effect on jigger fleas and is cheap and easy to use. It does not require sophisticated applicators or skilled personnel. It should be issued to heads of infested households or the community health worker assigned to the household for thorough dusting of floors, lower wall surfaces and compounds especially the areas commonly used by humans or pets for resting, once every three months.
This method can effectively control jigger populations, leading to eventual elimination. (Note: All chemical interventions carry a risk of toxicity to humans, other organism and the environment, especially the fragile aquatic environment. They should therefore be used judiciously).
17 National Policy
Guidelines on Prevention
and Control of Jigger
4.0. Guide for Regulation of Vector and Vermin
Control Operators
Depending on availability of resources, professional pest control outfits may be contracted by a stakeholder or health authority to carry out jigger extermination exercises in affected schools or households. County governments should enact legislation prescribing the criteria for the operations.
5.0. Guidelines for Equipment and Chemicals
i. Original knapsack sprayer — manual sprayer mounted on human back to spray
floors, walls and compounds;
ii. Motorized or mechanical sprayer — used on big exercises requiring intensive
labor such as the spraying of many infested households or entire schools with emulsifiable concentrates and where logistics of employing many spray men are unavailable;
iii. Swing fog machine — used to spray the exterior environment (compound) of
an already fumigated building. It oozes out chemical-smoke as against moisture released by knapsack or motorized sprayer. It can also be used to deplete or control other insect vectors and vermin in the compound;
iv. Other application methods include but are not limited to smoke generators,
fumigation tablets, and ready–to–use shaker canisters. Ready to use shaker
canisters can be very efficient for dispersing insecticidal dust on floors and on pet furs for the control of jigger fleas in the environment.
5.2. Chemicals
Jigger fleas have no known resistance to pesticides. The following commonly used pesticides preclude DDT which though highly effective as a controlled household spray, and has eliminated jiggers in some countries, is severely restricted in Kenya:
i. Pyrethrins and Pyrethroids – have faster knockdown effects and very long residual
action as a surface spray. Pyrethroids have faster knockdown effects on jigger fleas and
other insect vectors in the environment;
ii. Organophosphates– have extensively been used for Pest Control in agriculture. They
should be applied with caution in or around homesteads as they are toxic to untargeted
mammals and humans. Most organophosphates deteriorate rapidly and therefore pose
no problem of long-term environmental contamination or effects;
iii. Carbamate insecticides have a similar mode of action to the organophosphates.
Generally, carbamates such as Carbaryl (Sevin), Propoxur (Blattanex or Baygon) and
bendiocarb (Ficam) have even lower toxicity to mammals than most organophosphates.
Carbaryl has by far the largest use owing to its low mammalian toxicity and relatively
wide spectrum activity. Propoxur is also popular against household pests. Both are
Guidelines on Prevention
and Control of Jigger
relatively inexpensive and highly effective against jigger fleas in the environment. Carbaryl (Sevin dudu dust) and propoxur (Baygon dust) are safe, inexpensive and highly effective on jigger fleas when dusted on floors and domestic pets which harbor them;
iv. Botanicals: are natural insecticides derived from plants. Botanicals include
Pyrethrum, Rotenone, Ryania, Neem, Coconut oil and Nicotine. Pyrethrum is an oily
substance extracted from certain varieties of chrysanthemums plant. They are often
used in combination with synergists such as pieronys butoxide. They have faster knock-
down effects and usually of low toxicity to mammals like humans;
v. Fumigants: are gaseous pesticides whose vapors enter the pest system via
inhalation. Fumigants are used in food and grain storage facilities, but can be used for
other household pests including jigger fleas if dusting and spraying are not feasible due
to congestion of materials or furniture therein. Fumigants are toxic to all forms of life,
plants and animals. Faulty application may result into a catastrophe, killing non-targeted
organisms like pets. It is therefore, imperative that the operators check available
products literature to ensure a safe fumigation exercise;
vi. Rodenticides: are poisons which can be used to kill mice, which are reservoirs of
jigger fleas. They come in various forms such as granules, powder, cakes, etc. It is of
utmost importance that the jigger control operator knows and understands rodenticide
and adheres strictly to label instructions when applying them. Safety considerations
must be adhered to as most rodenticides are highly toxic and can be fatal if ingested in
very small quantity by humans.
6.0. Guidelines for Licensing of Vector and
Vermin Control Operators
To encourage private sector participation in Vector and Vermin Control, including jigger control and for sustainability, the County Governments (CG) shall license private Pest and Vector Control Outfits. Their Departments of Health shall regulate the private sector operators to ensure compliance with standards.
7.0. Health and Safety Considerations in
The use of pesticides (e.g. insecticides, acariscides and rodenticides) in jigger control requires technical skills, equipment, considerable financial input and above all, great care and precaution in application of the various toxic organic, inorganic, natural and synthetic chemicals. Numerous cases of pesticide poisoning among Public Health field workers have been reported all over the world including Kenya. Potential users at institutional, community and individual levels shall therefore:
19 National Policy
Guidelines on Prevention
and Control of Jigger
1. Undergo training in techniques for pesticide application in their various formulations
using a variety of equipment.
2. Pay special attention and care on PACKAGING, LABELLING, STORAGE, and
DISPOSAL OF USED PESTICIDE CONTAINERS.
3. Destroy all empty pesticide containers using a suitable incinerator or bury them in
an appropriate waste disposal site e.g. ash pit.
4. Use appropriate personal protective equipment such as respirators, nose masks,
goggles, face shields, gloves, and gumboots; long sleeve overall coats and washable hats, while carrying out jigger control operations.
5. Enforce observance of adequate personal hygiene through the provision of soap,
water and towel at all times during operations.
6. Ensure that no smoking, eating or drinking is undertaken during operations.
7. Undertake periodic biological monitoring especially cholinesterase levels if
organophosphate pesticide is frequently handled.
8. Ensure that all chemicals are kept out of the reach of children.
8.0. Tungiasis Treatment and Care
The surgical extraction of embedded sand fleas is very common but has several shortcomings. It is time-consuming, painful, often results in super-infections and secondary infections e.g. tetanus and HIV. Individuals may also abstain from the treatment due to the pain. This is also not an appropriate method to reduce environmental contamination by the human host. Additionally, the barrier function of the epidermis is not immediately reconstituted after sand fleas have been removed, so the sore produced by the surgical manipulation might temporarily increase the surface of the skin particularly susceptible to penetration. Treatment methods that kill the parasite insitu e.g. by toxic effect or suffocation might be more beneficial. Ultimately, prevention of infestation, rather than treatment of already embedded sand fleas, may interrupt transmission more effectively. These should target the various lifecycle stages of the flea in order to cut off transmission.
At the hospital, health centre, and dispensary and at the community level, the following clinical guidelines shall be used to treat jigger victims, curtail pathological sequels, rehabilitate them and generally combat ill-health caused by jigger infestations in the country.
1. No jigger victim maybe discriminated or refused treatment at health facilities due to
their jigger infestations.
2. Due to the secondary infection that can cause serious medical issues, the
recommended course of action is to sterilize the jigger wounds on feet and hands by soaking them in antiseptic solution e.g. Savlon, potassium permanganate or hydrogen peroxide for at least 15 minutes followed by topical application of petroleum jelly .The effects of the antiseptics on viability of embedded jiggers has not been subjected to rigorous studies but are thought to kill the embedded jiggers through suffocation when the infested feet are immersed in antiseptic solution for
Guidelines on Prevention
and Control of Jigger
at least 15 minutes. It is unclear whether the implied suffocation is attributable to the antiseptic or the water.
3. Flea repellants such as Deet, Zanzarin (coconut oil), neem and coconut oil
preparations, jojoba oil or aloe vera extract applied twice daily for a week have been shown to have provable programmatic value through the prevention of new infestations especially in households and areas of high tungiasis transmission. These repellants have an additional benefit of reversing clinical manifestations of tungiasis3.
4. For lesions in other parts of the body, surgical extraction of the flea followed by the
application of a topical antibiotic can help. Care should be taken to avoid tearing the flea during the extraction procedures as severe inflammation will result. The same will occur if part of the flea is left behind. Sterile equipment should always be used, as contaminated instruments could act as mechanical vectors for other pathogens to enter the body.
In general, there is no drug that has proven to be effective against embedded fleas but several products have varying degrees of efficacy:1. According to the Clinical Guidelines for Kenya, the aims of jigger treatment are to
suffocate the parasite and prevent secondary infections through immersion of feet in antiseptic solution for 15 minutes once a day for 2 weeks5.
2. The use of insect repellants is a very important public health intervention.
Therefore, patients whose infested feet and hands have been disinfected should be protected from re-infestation by use of approved repellants such as Zanzarin (combination of coconut oil, jojoba oil and aloe vera extracts) applied on feet up to ankle (2 to 3ml daily).
3. Immediate and continuous follow up of patient at home or school is necessary to
control the jigger fleas in the living or schooling environment.
4. Oral ivermectin: The anti-parasitic drug is considered by some in endemic areas to
be a panacea against embedded fleas. Mass treatment with ivermectin (2 doses of 200 μg/kg body weight 10 days apart) is said to have some benefits in preventing new infections but well-designed studies have not proved its efficacy.
5. Topical ivermectin (stromectol) and metrifonate have been somewhat successful,
but not enough to be significant.
6. For super infestations, trimethoprim, sulfamethoxazole, metronidazole, amoxicillin,
(with/without clavulanate) have been used successfully, though these treat only secondary infections.
7. Successful topical treatments also include cryotherapy (freezing of lesion using
liquid nitrogen) and electrodessication of the lesion.
8. Formaldehyde, chloroform, and municipal fluid (Kerol) can also be used topically,
but morbidity due to excess toxicity can result. Silicone oil (dimethicone) is a more effective and non-toxic remedy.
9. Occlusive (thick layer) petrolatum applied to infested lesions can also kill the
organism due to suffocation as the stigmata would be covered by the topical application.
10. At the same time, due to the high incidence of secondary infection, victims and
those at risk of tungiasis should get vaccinated against tetanus6.
21 National Policy
Guidelines on Prevention
and Control of Jigger
The World Health Organization (WHO) has listed tungiasis as a neglected disease of marginalized populations and has encouraged more significant research on the disease.
Therefore, more efficacious medications and new treatment regimes may be available for tungiasis in the future.
However, given the current unsatisfactory situation where tungiasis treatment regimes are of low efficacy, the adage "prevention is better than cure" rings true. The vector and vermin control principle of cutting the lifecycle of the vector or vermin; particularly at the larval stage is the most effective jigger prevention, control, elimination intervention. This should form the major focus for both levels of government and partners working in prevention and control of jiggers in the country.
10.0. Policy Recommendations
1. Tungiasis and jigger infestation is a self limiting health problem; therefore its
prevention and control interventions should target the infested households or schools for maximum impact. This is best accomplished through the ministry's community health strategy with its structure of community health volunteers.
2. Owing to the low efficacy of tungiasis treatment options, more efforts should be
geared towards prevention and control of jigger fleas to cut the transmission cycle. These include environmental and personal hygiene; chemical control of jigger fleas and the use of repellants.
3. Treatment of feet and other infested body parts with antiseptic solutions should
aim to prevent secondary infections and other complications such as disability and death.
4. Prevention of new infestations by use of approved insect repellants on feet and
hands can be a very effective tungiasis prevention strategy.
5. Administration of Tetanus Toxoid (TT) vaccine to jigger victims and those at risk
should be scaled up both at facility and household level.
6. Due to the social stigma, jigger victims are a hard-to-reach population with poor
health–seeking behaviour. Therefore, treatment camps should be organized regularly as an important outreach mechanism.
7. Follow-up of jigger victims identified at facility, outreach camp and at school level is
necessary for the control of infestation at the source i.e. household/school.
8. Promotion materials should aim to educate the public and particularly the most at
risk persons on the lifecycle of the jigger flea to enable them make decisions on prevention and control. This information should be complemented with information on hygiene and chemical control measures needed. It should ideally target schools in endemic areas.
Guidelines on Prevention
and Control of Jigger
9. Operational research, monitoring and evaluation should be incorporated in all jigger
prevention and control programs to track the implementation of their activities and ensure goals and objectives are being achieved or are on course. To achieve this, baselines of all infested households should be compiled by community health extension workers in all affected communities. Operational research should aim to improve existing tools and/or introduce new technologies that are both cost-effective and efficient in preventing and controlling tungiasis.
10. Division of Environmental Health, Vector Borne Diseases Control Unit (VBDU),
KEMRI, and research institutions will monitor insecticide resistance at regular intervals.
11. Industry and research institutions will explore alternatives to existing insecticides
for chemical control of jigger fleas and pharmaceutical products for control of embedded jiggers.
12. NEMA will monitor the impacts of various chemicals used in jigger prevention and
control while PCPB, KEBS and other regulatory bodies will monitor the quality of insecticides, pharmaceutical and other products for jigger prevention and control.
13. The ministry through DEH in collaboration with relevant stakeholders should
conduct regular cross-sectional surveys to determine prevalence and social-economic impacts of tungiasis.
14. At an organizational level, county and national governments should identify
potential actors and stakeholders and their specific activities. These should be consistent with these national guidelines. In particular, officers charged with vector control or environmental health at the county and national government levels should oversee all jigger prevention and control activities to ensure compliance with these guidelines.
15. The Ministry of Health, through the Division of Environmental Health, in
consultation with County Departments for Health and with input from the various other stakeholders, should review and revise these policy guidelines every 3 to 5 years to accommodate changes in disease epidemiology, take note of progress in implementation and consider incorporation of new research findings and lessons learnt.
16. Research on jigger prevention and control needs to be prioritized because literature
on the subject is scanty and there is need for additional authoritative knowledge on jiggers, their prevention and control. However, such research needs to be carried out in collaboration with medical research and academic institutions, with approval by the health ministry's ethics committee, for more rigour and credibility.
23 National Policy
Guidelines on Prevention
and Control of Jigger
1. MOH, Division of Environmental Health, Form 2B: Performance Contract report for
FY 2012-2013.
2. Bulletin of the World Health Organization vol.82 n.8 Aug. 2004, Selective mass
treatment with ivermectin to control intestinal helminthiases and parasitic skin
diseases in a severely affected population.
3. Marlene Thielecke, Vaomalala Raharimanga, Christophe Rogier, Manuela Stauss-
Grabo, Vincent Richard and Hermann Feldmeier, Prevention of Tungiasis and
Tungiasis-Associated Morbidity using the Plant-Based Repellent Zanzarin: A
Randomized, Controlled Field Study in Rural Madagascar, 2006.
4. Jörg Heukelbach, Thomas Wilcke, Margit Eisele and Hermann Feldmeier, Ectopic
Localization of Tungiasis, Am.J.Trop.Med.Hyg. , 67(2), 2002, pp. 214–216.
5. MOH, Clinical Guidelines for Kenya, 2002.
6. Jörg Heukelbach, Evelien Van Haeff, Babette Rump, Thomas Wilcke, Rômulo
César Sabóia Moura and Hermann Feldmeier, Parasitic Skin Diseases: health Care-
seeking in a Slum in North-East Brazil. Tropical Medicine & International Health
Volume 8, Issue 4, pages 368–373, April 2003.
7. Simon Kiprono Ruttoh, Denis Ochieng' Omondi and Nafula Inviolate Wanyama:
Tunga penetrans, a silent setback to Development in Kenya, Journal of Environmental
Science and Engineering, 2010.
Guidelines on Prevention
and Control of Jigger
12.0. Annexures
Annex A: Model Regulations for Pest Control Operators
1. Should be one that already provides services to residential homes, companies, food
premises, industries, offices and agricultural farms on fee for service basis;
2. Employ the services of a professional Pest and Vector Control technician who is
knowledgeable in all areas of vector and vermin control to provide environmentally
safe and effective control services;
3. Employ the services of a trained technician/repairer to maintain all equipment;
4. Provide a designated office for attending to customers who require Pest and Vector
Control services;
5. Provide a designated store for keeping equipment and chemicals. The store shall
be free from hazards, fire resistant, well ventilated, well lit, and shall be locked when
not in use. The store shall have adequate shelving arrangement and the floor shall
be made of impervious material;
6. Place a fire code sign on the door of the chemical store;
7. Ensure availability of fire extinguisher nearby;
8. Ensure appropriate ventilation in the chemical storage area;
9. Make available material safety data sheet for all chemicals stored;
10. Ensure that all chemicals are clearly labeled and handled with caution;
11. Conducts regular checks on all pesticides containers for signs of leakage, damage
and deterioration of contents;
12. Ensure that the pesticide application equipment is thoroughly cleaned and made
free of pesticide residue after use;
13. Ensure that equipment is well maintained and free of leaks;
14. Ensure that containers are emptied, thoroughly rinsed and rendered unusable
before disposal through the municipal waste management system or incineration (if
there is no restriction);
15. Make available to the operators, appropriate and adequate quantity of personal
protective equipment such as respirators, nose masks, goggles, gloves, boots, long
sleeve overall coats and helmets. Soap, water and towel shall be available at all
times for the use of operators;
16. Provide an appropriate vehicle for the pest control outfit. Drivers' cabin of the
vehicle must be separated from chemicals and equipment compartment;
17. Make available materials for keeping adequate record of pesticides available, date of
application, site address and pesticide used;
18. Issue appropriate certificate after each job is completed;
19. Stock spare parts for equipment maintenance.
Annex B: Recommended Criteria for Licensing Private Sector Participants
i. Provide evidence of registration of business name;
ii. Have a qualified technician in charge; the technician must hold the relevant
iii. State the type of Pest and Vector Control activity to be provided;
iv. Pay the requisite fees;
v. Renew the license annually;
vi. Attend regularly workshops/training organized by the CG on Pest and Vector Control.
The County Government shall inspect the office and stores of the private sector participant to ascertain the following:
• Adequate provision of equipment (compressed, mechanical, swing fog machines, etc).
25 National Policy
Guidelines on Prevention
and Control of Jigger
• Adequate storage of approved chemical and quality control. (List of approved
• Manpower outlay.
• Ensure submission of monthly reports of operations carried out to the CG.
Annex C: List of Common Chemicals for use in Domestic Pest and Vector
Control that can also be used to Control Jigger Infestations
Chemical
Other Activity Toxicity
spectrum, biodegradable,
spectrum, biodegradable,
spectrum, degradable,
Cyperme- synthetic
Microcide 2,2, dimethyl
This list of insecticides for use is not exhaustive. Persons handling pesticides shall take all necessary precautionary measures including the use of appropriate protective equipment anytime pesticides are handled.
Guidelines on Prevention
and Control of Jigger
Annex D: Jiggers Notification and Investigation Form
Republic of Kenya
MINISTRY OF HEALTH
JIGGERS (TUNGIASIS) NOTIFICATION AND INVESTIGATION FORM
COUNTY/SUBCOUNTY/WARD/VILLAGE/COMMUNITY UNIT Date _Name of Hospital/Health Centre/Dispensary/Clinic/Town/school _Name of patient Age _ Sex _ School Physical address Telephone Clinical History How long has the patient suffered from jiggers? Signs and symptoms:
1. Approximately how many jiggers or jigger wounds _2. Evidence of secondary infections (preuritis/ulceration/gangrenous)
Ability to walk (gait): normal _ abnormal
Treatment administered Final classification of jigger infestation:1. Mild2. Severe
Name Designation _
Signature _
NOTE: A Jigger Case investigation form must be completed by a health worker after treating or
examining a jigger patient and immediately sent to the Public Health Officer or Community Health
All households with jigger-infested patients must undergo fumigation or dusting with insecticidal
dust and all livestock and other domestic animals sprayed, dusted and removed from human living
27 National Policy
Guidelines on Prevention
and Control of Jigger
Annex E: Community Health Extension Worker Summary on Jiggers
Data element
Total households visitedTotal number of households infested with jiggersTotal population of the areaTotal children 5-12 yearsTotal elderly people 65 years Total children 5-12 years infested with jiggersTotal elderly people 65+ years infested with jiggers
Total jigger patients treated with antiseptic solution
Total number of households fumigated or dusted with insecticidal dust
Total number of households with floors improved by smearing or paving
Total households with adequate portable water
Total schools visitedTotal schools with paved classroom floorsTotal number of pupils wearing closed shoesTotal number of pupils infested with jiggersTotal number of infested pupils treated with antiseptic solutionTotal number of infested schools fumigated or dusted with insecticidal dustNumber of schools with adequate, portable water
People with jiggers referred
Data element
Number of jigger cases referred to health facility Number of jigger cases notified for follow upNumber of jigger cases followed up
Number of Jigger-related Deaths in the Month
Data element
Deaths 5- 12 yearsDeaths 65+ yearsDeaths in other age groupsTotal deaths
Guidelines on Prevention
and Control of Jigger
Source: http://www-scf.usc.edu/~kawright/Chigoe/National%20Policy%20Guidelines%20for%20Prevention%20and%20Control.pdf
CHAPTER 3 POINTS TO REMEMBER Acrosome : A small, sheathy structure at the end of a sperm.Blastula : A stage of embryogendesis which comes after morula and has ahollow fluid filled space called blastocoel.Endometrium : Innermost glandular layer lining the uterine cavity.Foetus : An advanced stage of embryo within the uterus.Gestation Period : A period between fertilisation of ovum and the birth of ababy.Hymen : A thin membrane partially covering the vaginal aperture.Implantation : Fixing of embryo/fertilized egg in uterus. It leads to pregnancy.Menarche : The beginning of first menstruation in female on attaining puberty.Menopause : Permanent cessation of menstrual cycle in female. It occursbetween the age 45 to 50 years in human female.Oogenesis : Formation and development of ova in ovary.Ovulation : Process of release of mature ovum (Secondary oocyte) from theovary.Parturition : Process of delivery of the foetus (Child birth).Puberty : A stage at which immature reproductive system of boy or girl becomesmature.Scrotum : A muscular pouch which houses two testes.
Brain Research 992 (2003) 69 – 75 Characterization of the GABAA receptor in the brain of the adult male bullfrog, Rana catesbeiana David M. Hollis*, Sunny K. Boyd Department of Biological Sciences, University of Notre Dame, Notre Dame, IN, USA Accepted 21 August 2003 Little is known about the properties of GABA receptors in the amphibian brain. The GABAA receptor is widespread in the mammalian brain,