Doi:10.1016/j.trstmh.2005.06.005
Transactions of the Royal Society of Tropical Medicine and Hygiene (2005)
99S, S1—S8
Public-private partnerships: an overview
Roy Widdus
Initiative on Public-Private Partnerships for Health (IPPPH), Global Forum for Health Research,
Received 16June 2005; accepted 17 June 2005
The development and marketing of medicines needed specifically to
combat diseases of the developing world are commercially unattractive because
developing world;
the populations concerned are among the poorest on earth. Partnerships which
bring together pharmaceutical companies, academics, not-for-profit organizations,
philanthropists, governmental and inter-governmental agencies are an increasingly
Product development
popular solution. These partnerships result in a complementarity of skills and
resources that can accelerate the development and delivery of new medicines
to those in need. Over the last 10 years or so, these public-private partnerships
(PPPs) have grown significantly in number and diversity. However, they tend to
Access public-private
cluster into two main groups: those dealing with product development (PD PPPs),
and those concerned with improving the access of new medicines to target pop-
ulations (Access PPPs). The Initiative on Public-Private Partnerships for Health
was set up four years ago to monitor the performance of these new partner-
partnerships for health
ships. After a series of studies of Access PPPs, it concluded that they provide
significant benefits with very few side effects, particularly in the case of tropical
2005 Published by Elsevier Ltd on behalf of Royal Society of Tropical Medicine and
portionately affect the poor' is perhaps a better
Infectious and parasitic diseases remain a major
In a vicious circle, poverty is a major cause of
cause of death worldwide The so-
health inequality in developing countries, and ill-
called ‘neglected diseases' affect the very poor
health perpetuates poverty. There are an estimated
in particular and therefore ‘diseases that dispro-
11 million premature deaths per year in the world's
poorest populations, and 80% of these are due to
infectious diseases (In
∗ Present address: Global Futures Health Network, Interna-
the age of globalization, many people still lack
tional Center Cointrin, Entrance G, 3rd Floor, 20, route de Pr´e-
access to essential medicines (
Bois, P.O. Box 1826, 1215 Geneva, Switzerland. Tel.: +41 22 799
4088; fax: +41 22 799 4089.
The UN Millennium Development Goals, adopted
in September 2000, set targets for progress in
0035-9203/$ — see front matter 2005 Published by Elsevier Ltd on behalf of Royal Society of Tropical Medicine and Hygiene.
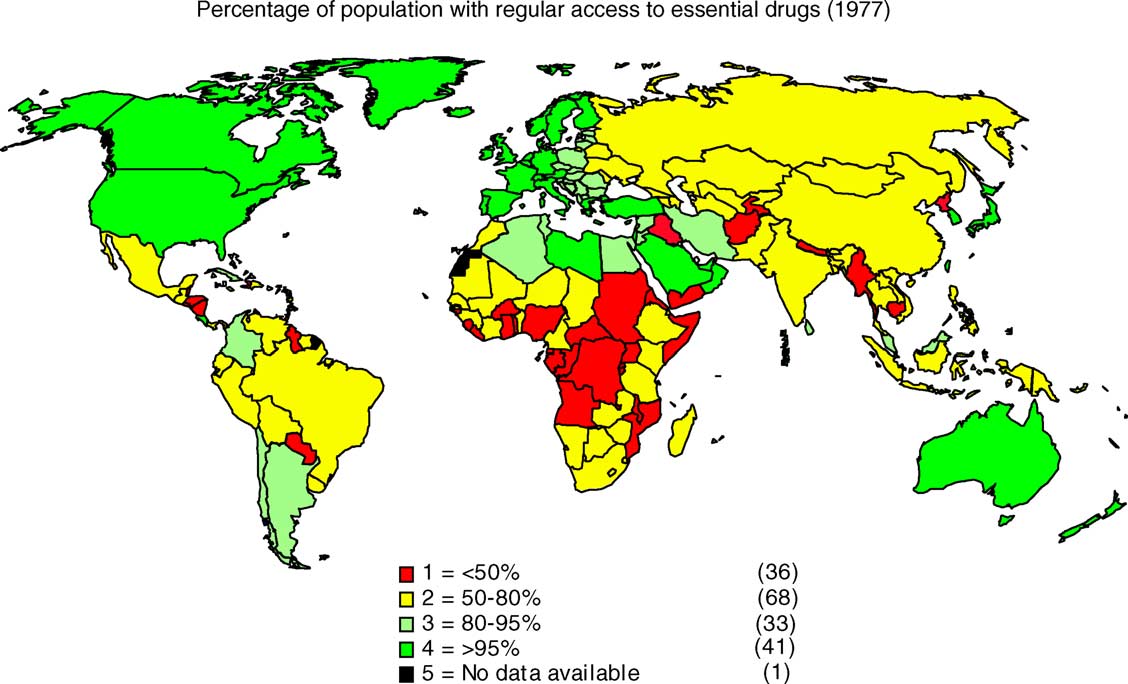
Figure 1 Many people still lack access to essential drugs.
tackling diseases of the developing world. These
The reality for the poor of the developing world
were to halt and begin to reverse the incidence
is very different. Products developed for global use
of HIV/AIDS, malaria and other major diseases by
have a relatively slow introduction into poor coun-
tries, usually caused by lack of planning and high
At present, however, it is very doubtful that
initial cost. Meanwhile, the development of prod-
these targets can be achieved in most of the poorer
ucts specifically needed to combat diseases dis-
countries. The problem is that the array of ‘tools'
proportionately affecting the poor has been sorely
currently available to meet the international tar-
neglected. Pharmaceutical companies are, after
gets on child mortality, HIV/AIDS, tuberculosis (TB)
all, commercial concerns with shareholders to con-
and malaria are inadequate for the poorer coun-
sider. New medicines are very expensive to develop.
Poor populations do not, by definition, provide a
There are no vaccines against HIV infection or
good return on this investment.
malaria and there is no vaccine to prevent the
The solution to this deadly conundrum is ‘part-
majority of TB cases (in adults). Existing diag-
nership'. Public-private partnership (PPP) brings
nostic tools or therapies for most diseases dis-
together funders such as philanthropists and gov-
proportionately affecting the poor are old and/or
ernmental and inter-governmental agencies with
difficult to use. First-generation vaccines against
academics, industry and not-for-profit organiza-
pneumococcal pneumonia may be too complex and
expensive for use in developing countries. Vac-
Public-private collaborations are needed to
cines against rotavirus diarrhoea are only just
tackle diseases of the developing world because
emerging. Other childhood killers lack preven-
no single sector — the for-profit private sector,
tion. Most drugs are threatened by increasing
the not-for-profit private sector or the govern-
ment agencies of the public sector — has all the
In an ideal situation, products developed for
skills and resources needed to make an impact on
global use move steadily along the research-
its own. Independent efforts by the public sec-
development-access continuum. Research is trans-
tor or by non-governmental organizations (NGOs)
lated into product concepts, these are devel-
have mostly failed. Public-private partnerships,
oped into proven products and manufacturing takes
however, result in a complementarity of skills and
place. The products go through regulatory approval
resources that can accelerate the discovery, devel-
to ensure consumer safety and are then introduced
opment and delivery of new products to those in
and used in well-functioning health systems.


2. Public-private partnerships — why
Over the last 10 years or so, PPPs have grown
significantly in number and diversity (The
Initiative on Public-Private Partnerships for Health
The 1990s saw the emergence of a number of trends
(IPPPH) was set up four years ago to undertake
conducive to the establishment of PPPs.
long-term monitoring of PPP performance with the
A systematic analysis of the global burden of dis-
aim of recommending best practices. The IPPPH is
ease highlighted ‘diseases associated with poverty'
part of the Global Forum for Health Research, a
and deficiencies in the tools to combat them.
small Swiss not-for-profit organization. The IPPPH is
Pharmaceutical companies faced rising research
funded by the World Bank, the Rockefeller Founda-
and development (R&D) costs, consolidation and
tion, the Gates Foundation and bilateral agencies.
greater competitive pressures. This increased their
aversion to commercially risky or unattractive
projects. Vaccines increasingly became ‘orphan'
products despite their importance, especially in
3. Definition of a public-private
developing countries. Meanwhile, the HIV/AIDS
pandemic drew global attention to the need for
greater action on the health needs of low and
Most PPPs comprise partners from three distinct
middle income countries. Last but not least, pub-
spheres. These are (i) the public sector, essen-
lic sector and public interest organizations began
tially governmental agencies and those institu-
to realise that they could achieve a positive
tions at the international level that are controlled
health impact if they could find a way of tap-
by governments, such as the WHO; (ii) the for-
ping pharmaceutical industry skills and resources.
profit sector, which includes the pharmaceutical
These factors, coupled with the emergence of dis-
and biotech companies; and (iii) the civil society
ease ‘champions' (see below) in the right place
sector, which includes academia, non-profit mak-
at the right time, have driven the growth of
ing organizations such as NGOs and philanthropic
The growth of PPPs has been helped by the estab-
Public-private partnerships are not legally joint
lishment of global coordinating and financing mech-
ventures in the business sense. Rather, they are
anisms such as the Global Alliance for Vaccines and
joint ventures sharing a set of attributes, the most
Immunization and the Vaccine Fund (GAVI/VF), Roll
important of which is a shared objective. The moti-
Back Malaria (RBM), the Stop TB Partnership and the
vations of the partners vary, as do their contribu-
Global Fund for AIDS, TB and Malaria. These create
tions and benefits they expect to receive in return.
a significant ‘market' by funding the uptake of new
Public-private partnerships involve shared decision
making and risk taking.
Figure 3 Collaborative relationships between public and private sectors.
4. Public-private partnerships today
lowed and laid the groundwork for IAVI (
Today there are over 100 ventures involving phar-
Medicines for Malaria Venture, founded in 1999,
maceutical or other health sector companies that
was the first drug development PPP. Two individ-
can be described as PPPs. They are concerned with
uals, Win Gutteridge and Robert Ridley, were the
diverse topics including research, global coordi-
‘champions' here. Both had pharmaceutical indus-
nation and financing mechanisms, health system
try experience of product development and the
strengthening, public education, advocacy and reg-
portfolio approach. Gutteridge and Ridley initiated
ulation, quality and standards. The majority, how-
discussions between the Geneva-based Special Pro-
ever, tend to cluster into two main groups: those
gramme for Research and Training in Tropical Dis-
dealing with the development of drugs and vac-
eases (TDR), industry and malaria specialists. The
cines, the so-called product development partner-
new venture was supported by various other orga-
ships (PD PPPs), and those concerned with improv-
nizations, including the Rockefeller Foundation and
ing access to medicines (Access PPPs). A third small
the Global Forum for Health Research
group, noted above, includes the global coordina-
tion and financing mechanisms
There are now some 20 PD PPPs. Some have only
small portfolios. However, the older ventures have
at least five or six years of operational experience
4.1. Public-private partnerships for product
and sizable portfolios. Their emergence was orig-
inally fostered by the Rockefeller Foundation and
subsequently by substantial funding from the Gates
Public-private partnerships for the development of
new products to combat diseases of the develop-
Because of the variation among PD PPPs, they do
ing world began to emerge in the mid-1990s. There
not all work in an identical fashion, but there are
had, of course, been earlier sporadic collabora-
broad similarities which allow us to define a ‘typi-
tion on an ad hoc basis around individual candidate
cal' operation. All need to move candidate products
products between public sector agencies and phar-
through the R&D continuum as quickly and econom-
ically as possible (They
The new PD PPPs are different. Instead of taking
may take on candidate products at any point in that
a specific candidate product as their starting point,
continuum. However, few PD PPPs fund activities
these new partnerships survey the field and then
translating basic research into candidate products.
promote the parallel development of a range of
All candidate products must go through a num-
different products. This ‘portfolio' approach, bor-
ber of development stages requiring certain types
rowed from the pharmaceutical and venture capital
of testing. At the end of each stage, each candi-
fields, is designed to manage the risk of failure
date is re-assessed. Those with promise move on
accompanying any individual project.
to the next stage, while those with problems such
The first PD PPP addressing infectious diseases
as low efficacy or toxicity are abandoned. Because
was the International AIDS Vaccine Initiative (IAVI),
so many drug candidates fail, it is cost-efficient to
established in 1996. Some features of IAVI's and
make the decision to abandon a project quickly.
Medicines for Malaria Venture's (MMV) approach can
Public-private partnerships for product develop-
be seen in the contraceptive field, around the mid-
ment with a portfolio of candidate products at dif-
1990s (The IAVI was the
ferent stages can routinely replace those that have
brainchild of Seth Berkley, a public health epidemi-
been terminated.
ologist with experience of the early HIV/AIDS epi-
Each step of testing candidate drugs requires
demic in Uganda. Berkley was then working at the
both expertise and resources which may not exist
Rockefeller Foundation. He realised that in order
within the PD PPPs themselves: e.g. specialized
to meet a global health need on this scale both
laboratory equipment, animal models or access to
philanthropic funding and industry expertise were
human populations at risk of the target disease.
needed. He also saw that problems surrounding the
Public-private partnerships for product develop-
accessibility of new products to poor populations
ment, unlike large pharmaceutical companies, do
had to be addressed in order to achieve a significant
not generally conduct all their activities ‘in house'.
health impact. Berkley persuaded the Rockefeller
Instead they act as managers, bringing together
Foundation to convene a meeting entitled ‘Accel-
the needed expertise and resources in collabora-
erating the development of preventive HIV vaccines
tive project teams. These teams, drawn from phar-
for the world'. Further meetings, co-sponsored by
maceutical companies and other organizations, are
the foundation and by the Fondation Merieux, fol-
contracted to carry out specified testing steps in

Table 1 Diversity — the legal status of various partnerships addressing health problems
Downloaded from http://trstmh.oxfordjournals.org/
at Emory University on March 29, 2013
their own facilities, physically and organizationally
In most cases, national programme managers
distant from the PPP. This method, which requires
dealt primarily with the WHO and had minimal
lower investment in the PD PPP's own staff and
contact with the participating pharmaceutical
infrastructure and promotes flexibility, has come to
companies. No specific challenges arose from the
be known as ‘virtual R&D'.
involvement of the pharmaceutical companies.
By using collaborators, PD PPPs save time and
In fact, there were several instances of benefits
money, but pharmaceutical companies and other
beyond the donation or discounting of drugs, e.g.
contributors also benefit in various ways. The aim
in contributions to capacity building.
is to promote a ‘Win-Win' situation for everyone
Governments and clinicians welcomed the drug
concerned (see Nwaka, this supplement). ‘Virtual
access PPPs. Without them, the countries stud-
R&D' places extra management demands on the
ied would generally struggle to afford the drugs.
PD PPP, but it is certainly cost-effective. A major
The widely-held conclusion at country and global
consultation in April 2004 concluded that the older
level was that these drug access PPPs have assisted
portfolio-based product development partnerships
the poor to obtain necessary drugs. The studies
using the collaborative approach had shown signs
found no evidence of unreasonable conditionalities,
of progress, but funding needed to be expanded
impaired national ownership, distortion of national
Although they draw upon
or district priorities, or unhelpful reallocation of
skills and procedures that are well established in
human and financial resources at central, district
the commercial sphere, these PD PPPs are essen-
or community levels.
tially ‘social experiments'. ‘Best practices', proven
However, the research showed that continued
by the delivery of products, are not yet avail-
support by donors in the maintenance as well as
able. However, the development of comparative
the intensive phases of elimination/control is vital
performance measures will become necessary in
if resurgence of disease is to be avoided. Likewise,
the near future as judging ‘success' is important to
Access PPPs must ensure that their operations are
integrated with the district health system within
disease-endemic countries from the outset. Fail-
ure to do this resulted in the resurgence of African
4.2. Access public-private partnerships
trypanosomiasis (sleeping sickness) in Uganda when
project staff withdrew after control was achieved.
These are partnerships addressing access to drugs
In the case of donations or discounted pricing for
in low to middle income countries. They are based
access to HIV/AIDS drugs, where multiple play-
on pharmaceutical industry donations or discounted
ers or programmes existed, there was a need for
pricing. Many are for tropical diseases and these
more coordination and more support to countries,
are often embedded within larger collaborations,
particularly from international organizations, to
sometimes for the elimination of a particular dis-
reduce fragmentation and improve understanding
Many of these access partnerships pre-date the
emergence of the PD PPPs. It is not generally rec-
ognized how successful the Access PPPs have been
so far. The oldest, the Mectizan® donation pro-
gramme for onchocerciasis (river blindness) in West
Africa, has reached 40 million people in the last
Over the last 10 or 15 years PPPs have made signif-
decade. Meanwhile, GSK's donation of albenda-
icant progress in tackling diseases that dispropor-
zole within the Global Alliance for the Elimination
tionately affect the poor.
of Lymphatic Filariasis (GAELF) reached 80 mil-
The drug access PPPs, such as the Mectizan®
lion people in 2003 alone, through mass community
donation programme for onchocerciasis in West
Africa and the donation of albendazole within
A series of studies of access partnerships under-
the GAELF, have already achieved, or are well
taken by the IPPPH in Botswana, Sri Lanka, Uganda
on the way to achieving, significant public health
and Zambia in 2003—2004
impacts. They have helped the poor to access
found that these PPPs have significant benefits with
necessary drugs without distorting health priorities
very few side effects, particularly in the case of
at national or local level.
tropical diseases. The studies concluded that phar-
Product development public-private partner-
maceutical company involvement in tropical dis-
ships, meanwhile, have made an impressive
ease Access PPPs substantially improved drug avail-
start since they began to emerge in the mid-1990s.
ability in the four study countries.
There are now significantly more projects underway
aimed at developing new drugs to combat diseases
Nwaka, S., Ridley, R., 2003. Virtual drug discovery and develop-
associated with poverty. What sort of public health
ment for neglected diseases through public-private partner-
impact today's PD PPPs will eventually achieve,
ships. Nat. Rev. Drug Discov. 2, 919—928.
only time can tell. However, for millions of the
Ridley, R.G., Gutteridge, W.E., Currat, L.E., 1999. New
medicines for malaria: A case study of the establishment of
world's poorest people whose deadly afflictions
a public/private sector partnership. Presented at 3rd Global
have been ignored for so long, it is truly a great
Forum for Health Research, Geneva.
step in the right direction.
Rockefeller Foundation, 1995a. Summary report and recommen-
dation of an international ad hoc scientific committee. 27—28
October 1994. Le Val de Grˆace, Paris, France.
Rockefeller Foundation, 1995b. Summary report and recommen-
dations of an international meeting: Financial and structural
issues. 17 August 1995. New York.
Caines, K., Lush, L., 2004. Impact of Public-Private Partnerships
Widdus, R., White, K., 2004. Combating Diseases Associated
Addressing Access to Pharmaceuticals in Selected Low and
with Poverty: Financing Strategies for Product Develop-
Middle Income Countries: A Synthesis Report from Studies
ment and the Potential Role of Public-Private Partner-
in Botswana, Sri Lanka, Uganda and Zambia. Initiatives on
ships. Initiative on Public-Private Partnerships for Health,
Public-Private Partnerships for Health, Geneva.
Gwatkin, D., Guillot, M., 2000. The Burden of Disease among the
WHO, 2004. World Health Report. World Health Organization,
Global Poor. The World Bank, Washington, D.C., p. 44.
Source: http://web1.sph.emory.edu/users/hpacho2/PartnershipsMaize/Widdus_2005.pdf
APPLICATION MANUAL 2016 09 GENER AL INFORMATION 86 Machines, Tools, and Aids 14 General Product Information 21 Swarovski Products and Suitable Application 100 Quick Assistance101 Swarovski Hotfix Selector 23 SOLDERING, PL ATING, AND STONE SET TING SEWING, EMBROIDERY, AND HAND APPLICATION 24 Machines, Tools, and Aids25 Suppliers 112 Product Overview 112 Machines, Tools, and Aids
JBC Papers in Press. Published on May 31, 2011 as Manuscript M111.253674 OPTOGENETIC CONTROL OF MOTOR COORDINATION BY Gi/o PROTEIN-COUPLED VERTEBRATE RHODOPSIN IN CEREBELLAR PURKINJE CELLS. Davina V. Gutierrez2, Melanie D. Mark1, Olivia Masseck1, Takashi Maejima1, Denise Kuckelsberg1, Robert A. Hyde2, Martin Krause1, Wolfgang Kruse1, and Stefan Herlitze1,2