Untitled
Journal of Infectious Diseases Advance Access published June 11, 2014
Frailty in People Aging With HumanImmunodeficiency Virus (HIV) Infection
Thomas D. Brothers,1 Susan Kirkland,2 Giovanni Guaraldi,3 Julian Falutz,4 Olga Theou,1 B. Lynn Johnston,5 andKenneth Rockwood6,7
1Geriatric Medicine Research, and 2Departments of Community Health and Epidemiology and Medicine, Dalhousie University, Halifax, Nova Scotia,Canada; 3Department of Medical and Surgical Sciences for Adults and Children, Clinic of Infectious Diseases, University of Modena and Reggio Emilia,Modena, Italy; 4Chronic Viral Illness Service, Division of Infectious Diseases and Division of Geriatrics, McGill University Hospital Center, Montreal,
Quebec, Canada; 5Division of Infectious Diseases, and 6Division of Geriatric Medicine, Dalhousie University, and 7Centre for Health Care of the Elderly,Capital District Health Authority, Halifax, Nova Scotia, Canada
The increasing life spans of people infected with human immunodeficiency virus (HIV) reflect enormous treat-ment successes and present new challenges related to aging. Even with suppression of viral loads and immunereconstitution, HIV-positive individuals exhibit excess vulnerability to multiple health problems that are not
AIDS-defining. With the accumulation of multiple health problems, it is likely that many people aging withtreated HIV infection may be identified as frail. Studies of frailty in people with HIV are currently limitedbut suggest that frailty might be feasible and useful as an integrative marker of multisystem vulnerability,for organizing care and for comprehensively measuring the impact of illness and treatment on overall healthstatus. This review explains how frailty has been conceptualized and measured in the general population, crit-ically reviews emerging data on frailty in people with HIV infection, and explores how the concept of frailtymight inform HIV research and care.
Keywords. HIV; frailty; aging; risk assessment; geriatric assessment; chronic infectious disease; chronic viral illness.
AGING WITH HIV INFECTION
some cancers, as well as age-associated immunologicchanges and chronic inflammation [Each involve
Effective therapies have transformed human immuno-
different physiological systems and etiologies yet are all
deficiency virus (HIV) infection into a chronic illness
strongly age-associated in the general population. While
]. As people with HIV live longer, aging-related chal-
HANA conditions are more common among HIV-pos-
lenges are arising. Despite complete suppression of viral
itive individuals who are older, have more severe HIV
load and immune recovery, HIV-positive individuals
disease, and who have longer duration of antiretroviral
are more vulnerable to poor health than HIV-negative
treatment and toxicity, these factors do not completely
individuals []. This vulnerability is characterized by
explain differences in risk and survival [].
higher risk of several common, age-related health prob-
Among people without HIV, aging and the accumu-
lems, even after adjustment for established risk factors.
lation of age-related health problems are also highly
These conditions, termed HIV-associated non-AIDS
heterogeneous processes. Although people generally ac-
(HANA), include cardiovascular disease, osteoporosis,
cumulate health problems with age, individuals of the
metabolic disorders, hepatic and renal diseases, and
same age can experience very different levels of health.
Geriatricians introduced the term "frailty" to describethis variability. Frailty represents the cumulative effects
Received 23 December 2013; accepted 23 April 2014.
Correspondence: Kenneth Rockwood, MD, Division of Geriatric Medicine, Dal-
of age-related deterioration in multiple physiological
housie University, 1421-5955 Veterans' Memorial Lane, Halifax, NS B3H 2E1, Can-
systems and homeostatic mechanisms, resulting in
greater vulnerability to stressors , Frail individuals
The Journal of Infectious Diseases The Author 2014. Published by Oxford University Press on behalf of the Infectious
often present with nonspecific health complaints, fluc-
Diseases Society of America. All rights reserved. For Permissions, please e-mail:
tuating disability, falls, and delirium and are at higher
risk for multiple adverse outcomes, including longer
Frailty in HIV Infection • JID • 1
hospital stays, postoperative complications, poor responses to
cumulative deficit model The phenotype views frailty as a
vaccination, functional decline, and death ].
clinical syndrome arising from a "cycle of frailty" composed
With the accumulation of multiple health problems, it is like-
of chronic undernutriton, sarcopenia, and weakened strength
ly that many people aging with HIV may be identified as frail
and exercise tolerance. It suggests that frailty pathophysiology
]. The concept of frailty could provide a useful tool to measure
is distinct from aging or other disease processes ]. Other fac-
and communicate the complexity of aging and vulnerability in
tors, such as cognitive impairment, have been suggested as fur-
people living with HIV, inform the development of therapies,
ther phenotypic characteristics of frailty [].
and guide the delivery of care. This review explains how frailty
The cumulative deficit model (first proposed by members of
has been conceptualized and measured in the general popula-
our group) views frailty as a state of vulnerability, rather than a
tion, critically reviews emerging data on frailty in people living
syndrome. It suggests that frailty arises from the cumulative effects
with HIV, and explores how applying the concept of frailty to
of nonspecific age-related health deficits and does not have a
research and care might benefit people living with HIV.
unique pathophysiology but rather is related to the aging process[. As people accumulate health deficits and homeostatic mech-
FRAILTY IN THE CONTEXT OF HIV
anisms begin to fail, those who are frail exhibit excessive changes
in health in response to even minor further insults []. Under this
Investigators have begun investigating frailty among people
model, frailty has been proposed to describe the overall health
with HIV to identify individuals more vulnerable to disease
state of an individual and therefore serve as an integrative marker
progression and death and to measure the effects of illness
of biologic aging, as opposed to chronological age , ].
and treatment on health status [, . However, frailty is
Studies applying both frailty models have identified associa-
not yet well understood in the context of the highly active
tions between increasing severity of frailty and age-related dete-
antiretroviral therapy (HAART) era, where most HIV-positive
rioration in multiple systems, including immunosenescence and
individuals now experience significant immune recovery, unde-
chronic inflammation [, ], which may be particularly rele-
tectable HIV viral load, and primarily HANA clinical manifes-
vant in people with treated HIV [, , ].
tations , ]. Neither CD4 count nor viral load appear to beuseful surrogate markers of vulnerability in this immune-recon-
MEASURING FRAILTY
stituted population, whereas frailty is strongly associated with
HANA conditions and disability and might be a
Multiple measures exist to identify and measure frailty. Some
more sensitive indicator of health changes , ]. Age-related
are based on clinical judgment or a single item (eg, walking
and HANA conditions have been associated with both immune
speed), but most scales assess multiple domains of age-related
activation (eg, soluble CD14 and CD163, CD16+ monocytes,
health and grade frailty by counting the number of deficits in-
HLA-DR+/CD38+ CD8+ T cells) and immune senescence
dividuals have acquired One commonly used scale, based
markers (eg, terminally differentiated CD45RA + CCR7−
on the frailty phenotype [identifies frailty by the presence of
CD4+ T cells), as well as inflammatory circulating cytokines
3 deficits out of 5 specific measures originating from the Car-
(eg, interleukin 6, tumor necrosis factor α [TNF-α]) [,
diovascular Health Study (an existing prospective cohort
]. Frailty is associated with both CD4 count and viral load
study): self-reported unintentional weight loss >10lbs or record-
], yet relationships between frailty and markers of immune
ed weight loss ≥5% in a year, measured slow walking speed,
senescence and activation among HIV-positive individuals
measured weak grip strength, self-reported exhaustion (3-4
have not been established. Although the clinical spectrum of
days per week or most of the time), and low activity/energy ex-
HIV disease differs whether individuals experience immune de-
penditure (assessed by Minnesota Leisure Time Questionnaire)
ficiency or immune activation, frailty might emerge in the con-
[The frailty phenotype scale has been widely applied and
text of both profiles. A hypothetical representation of the
extensively validated in its ability to identify people at increased
association between frailty, HANA, and immune system dysre-
risk for a range of adverse outcomes [
gulation is depicted in Figure Causal pathways between these
Another commonly used scale, the "frailty index," counts the
factors are not yet understood, in part because most studies in-
number of deficits individuals have accumulated out of various
vestigating HANA or frailty in HIV have been cross-sectional.
health measures and presents them as a proportion [, ].
In contrast to the phenotypic approach, any measure can be
included in a frailty index if it is generally related to age andpoor health, and if the group of items covers multiple physio-
While "frail" is commonly used to describe vulnerable older
logical systems. When at least 30 items are included, the propor-
adults, there is no consensus on the best way to define and iden-
tion of deficits accumulated appears more informative than the
tify frailty systematically [Two conceptual models inform
specific nature of those deficits. Though the effect of each indi-
most approaches to frailty: the phenotype model and the
vidual deficit may be small, their cumulative effects can be large.
2 • JID • Brothers et al
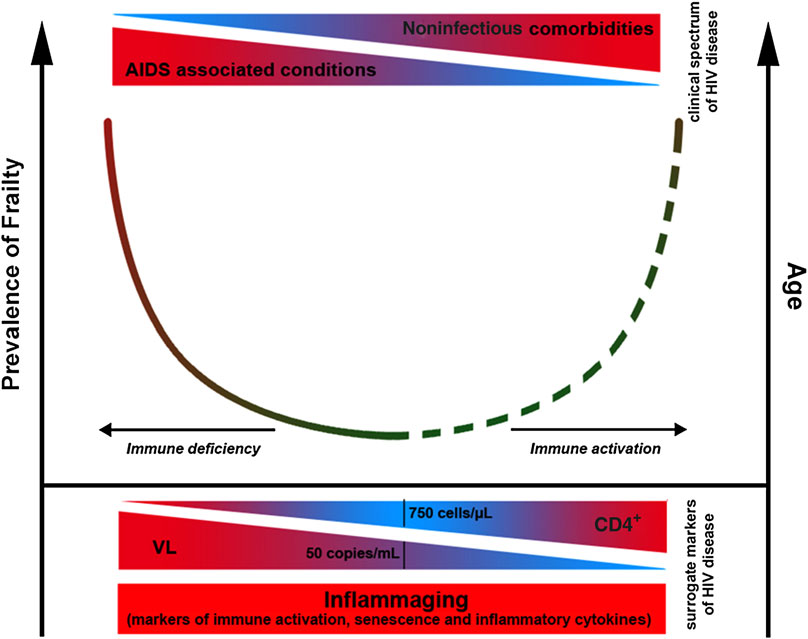
Hypothetical association between frailty prevalence, HANA conditions, and immune system dysregulation. Presented at 4th International Work-
shop on HIV and Aging, 30–31 October Baltimore, MD ]. Abbreviations: HANA, HIV-associated non-AIDS; HIV, human immunodeficiency virus.
This reinforces the notion that health problems in the same in-
accumulated diverse deficits in health; they might, however, be
dividual rarely arise independently from one another [,
relatively cumbersome to construct [, ]. Parsimonious
Each frailty index can make use of different available measures,
scales can be quicker to apply but often require specific mea-
including functional limitations, comorbidities, cognition, and
sures (eg, grip strength measured by dynamometer) and
affect ]. This approach has been operationalized clinically
might overlook people with different health problems. Modifi-
using data from comprehensive geriatric assessments and rou-
cations to such scales are common, especially replacing perfor-
tine medical records
mance-based measures (eg, walking speed) with self-reported
Many other frailty scales exist, often including more items
measures (eg, reported difficulty walking), or using different cri-
than the 5 specified by the frailty phenotype but fewer than
teria for performance-based measures (eg, loss of >10lbs in past
the 30 suggested by the frailty index ]. By counting health
year vs loss of >5% of body weight in past 6 months), yet the
deficits across multiple physiologic systems, frailty scales are
validity of such modifications is unknown
each able to identify individuals vulnerable to adverse outcomesand to do so better than chronological age alone [, ]. Al-though scales differ in the number and nature of deficits they
MEASURING FRAILTY IN HIV-POSITIVE
count, people who have accumulated more deficits are more
likely to be vulnerable and therefore more likely to be frail]. Different scales also demonstrate remarkable consistency
All published studies of frailty in HIV infection use frailty scales
in characteristics, including the nonlinear relationship between
composed of a limited number of specific health measures, fol-
frailty severity and age, greater frailty in women than same-aged
lowing the phenotype approach (Table ). For instance, analyses
men, and higher risk of death in men than women of equal
of the Multicenter AIDS Cohort Study (MACS) used a frailty
scale based on 4 self-reported deficits: weight loss, exhaustion,
However, as they include different criteria, frailty scales vary
impaired physical activity, and difficulty walking [One
in ability to predict outcomes and in operational feasibility in
study used a single measure of unexpected weight loss to define
different settings ]. Frailty scales that include more measures
frailty ]. No published studies of frailty in people with HIV
can more sensitively grade vulnerability and track improvement
have used the cumulative deficit/frailty index approach, or
and decline and are less likely to overlook individuals who have
scales based on clinical judgment.
Frailty in HIV Infection • JID • 3
Deficits Included in Different Frailty Scales Applied to People Living With HIV
Inclusion Criteria
Deficits Included in Frailty Scale
Based on frailty phenotype scale:
Urban, community-
Age 18+; no clinical AIDS
Considered frail if 3
Weight loss: ‘Since your last visit (6 mo
based cohort of men
ago), have you had unintentional weight
who have sex with
loss of at least 10 pounds?'
Exhaustion: ‘During the past 4 wks, as
a result of your physical health, have
you had difficulty performing your work
or other activities (for example, it took
Low activity: ‘Does your health nowlimit you in vigorous activities, such asrunning, lifting heavy objects,participating in strenuous sports?'
Slowness: ‘Does your health now limit
you in walking several blocks?'
Urban, community-
Age 18+; either HIV−, or
Considered frail if 3
Weight loss: ‘Since your last visit have
HIV+ receiving ART
you had unintended weight loss of at
least 10 pounds?'
Exhaustion: ‘During the past 4 wks, as
a result of your physical health, have
you had difficulty performing your work
or other activities (for example, it took
Low activity: ‘Does your health nowlimit you in vigorous activities, such asrunning, lifting heavy objects,participating in strenuous sports?'
Slowness: Timed 4 m walk
Weakness: Grip strength measuredwith dynamometer
Urban, community-
Age 13+; receiving ART;
Considered frail if 3
Weight loss: ≥10 pounds in past year,
based HIV-positive
participants with ‘missing
self reported and confirmed by physical
female cohort in five
limbs, prostheses,
paralysis, or assistive
Exhaustion: ‘based on responses to
devices' were excluded
two items from the CES-D scale'
from walking speed and
Low activity: A modified version of the
grip strength tests and
Minnesota Leisure Time Activities
assigned missing values
Questionnaire ‘capturing intensity andduration of 18 activities that range fromwork to child care'
Slowness: Timed 4 m walk
Weakness: Grip strength measuredwith dynamometer
Urban, outpatient clinic
Age 18+; participants with
Considered frail if 3
Weight loss: >10 pounds in past year
convenience sample
any pain, arthritis,
or ≥5% of previous year's body
tendonitis, or carpal
weight, unintentionally, based on
tunnel syndrome were
excluded from grip test
Exhaustion: Answering ‘occasionally
and assigned missing
(3–4 d)' or ‘most of the time (5–7 d)' to
values; participants with
either ‘How often have you felt that
missing limbs, paralysis,
everything you did was an effort' or
or needing assistive
‘How often have you felt that I could not
device were excluded
from walking speed test
Low activity: Answering ‘yes, limited a
and assigned missing
lot', when asked ‘whether their health
limits vigorous activities such asrunning, lifting heavy objects'
Slowness: Timed 15 ft walk, stratifiedby gender and height
Weakness: Grip strength measuredwith dynamometer, stratified by genderand body mass index
4 • JID • Brothers et al
Table 1 continued.
Inclusion Criteria
Deficits Included in Frailty Scale
Urban, community-
Age 18+; history of injecting
Considered frail if 3
Weight loss: ≥5% of body weight since
last visit (ranged from 5 to 12 mo),
preset; ‘prefrail' if
based on physical exam
history of injecting
Exhaustion: Answering ‘moderate' or
‘most of the time' to either ‘During the
past week, I felt everything I did was an
effort' or ‘During the past week, I couldnot get going'
Low activity: Answering ‘limited a lot',when asked ‘Does your health nowlimit the kinds or amount of vigorousactivities you can do, like lifting heavyobjects, running, or participating instrenuous sports?'
Slowness: Timed 4 m walk; deficit
assigned to lowest 20% of participantsstratified by gender and height
Weakness: Grip strength measuredwith dynamometer; deficit assigned tolowest 20% of participants stratified bygender and body mass index
Urban, outpatient clinic
Considered frail if 3
Weight loss: ≥10 pounds in past year,
convenience sample
unintentionally, based on physical exam
Exhaustion: Answering ‘3 to 4 d' or ‘mostof the time' to either ‘How often in thelast week did you feel that everything wasan effort' or ‘ . . I could not get going.'
Low activity: Weighted score ofkilocalories expended per week asmeasured by Minnesota Leisure TimeActivity Questionnaire
Slowness: Timed 15 ft walk, stratifiedby gender and height
Weakness: Grip strength measuredwith dynamometer, stratified by genderand body mass index
Urban, community-
Age 30+; no opportunistic
Considered frail if 3
Weight loss: >10 pounds in past year,
based HIV-positive
infections or symptoms
or ≥5% of previous year's body weight,
unintentionally, based on clinic records
participants with pain or
Exhaustion: Answering ‘occasionally
arthritis of dominant hand
(3–4 d)' or ‘most of the time (5–7 d)' to
were excluded from grip
either ‘How often have you felt that
strength test and
everything you did was an effort' or
assigned missing values;
‘ . . that I could not ‘get going''
participants with paralysis
Low activity: Answering ‘yes, limited a
or needing assistive
lot', when asked ‘whether their health
device were excluded
limits vigorous activities such as
from walking tests and
running, lifting heavy objects.'
assigned missing values.
Slowness: Timed 6 m walk, stratified bygender and height
Weakness: Grip strength measuredwith dynamometer, stratified by genderand body mass index
All individuals receiving
Age 45–65; taking effective
Considered frail if 3
Weight loss: ≥4.5 kg in past year, or
ART for at least 6 mo; at
≥5% of previous year's body weight,
least one clinic visit with
unintentionally, self reported and
outpatient clinic at a
plasma HIV RNA <48
verified by records when available
copies/mL, and no visit
Exhaustion: 3-4 times per week of
with plasma HIV RNA
feeling ‘everything I do is an effort' or
>200 copies/mL in prior
‘sometimes I just cannot get going.'
Low activity: Self-report of being
‘limited a lot' in vigorous physicalactivities on the SF-36 questionnaire
Slowness: Timed 4.5 m walk, stratifiedby gender and height
Weakness: grip strength measuredwith dynamometer, stratified by genderand body mass index
Frailty in HIV Infection • JID • 5
Table 1 continued.
Inclusion Criteria
Deficits Included in Frailty Scale
Participants recruited
Age 20–40 or 50+; English
Considered frail if 3
Weight loss: >10lbs unintentional
for a pilot clinical trial
speaking; on stable ART
weight loss (time period unspecified)
for 12 wks or not
Exhaustion: Fatigue Severity Scale
anticipating initiating ART
for 6 wks; no intercurrent
Low activity: POMS activity scale score
acute infection, active
psychiatric illness, active
Slowness: Timed Gait Test (10
neurologic disease,
yards × 2) >11 s
current delirium or
Weakness: Grip strength >1 SD below
intoxication, active drug or
alcohol overuse, orpregnancy
Based on other frailty scales:
Urban, hospital based
Age 50+; receiving
Considered frail if
Physical Performance Test score of 18
HIV clinic outpatients
antiretroviral therapy for
3+ mo and continuing;
Peak oxygen uptake of 11 to 18 mL/kg
able to ambulate without
assistive devices; no
Difficulty with one activity of daily living
AIDS-defining illnesses
(ADL) or two or more instrumental
for 6 mo; no ‘severe
cardiopulmonary illness,
severe anemia, significantorthopedic orneuromuscularimpairments, renal failure,cirrhosis, significantcognitive or sensoryimpairments, untreateddepression, unstablemanic or psychoticdisorder, or active
20 patients selected
Participants had identified
Limitations with basic activities of daily
from outpatient clinic
problems in multiple
severely frail if 3
Limitations with instrumental activities
of dialing living
moderately frail if
‘hearing and visual screening'
frail if 1 deficit
‘mobility problems'
All patients newly
Considered frail if
Unexpected weight loss
diagnosed with HIV
infection at tertiary
care hospital inKolkata from 2008 to2012
All HIV-positive US
veterans receiving
care in the Veterans
FIB-4 (a measure of liver fibrosis):
(years of age × AST)/platelets in 100/
L × square root of ALT)
Estimated glomerular filtration rate:
creatinine)−1.154 × (age)−0.203 × 1.21 ifBlack
Hepatitis C status
Abbreviations: ART, antiretroviral therapy; HIV, human immunodeficiency virus.
A recently introduced measure of health status in people
The VACS index is a prognostic tool made up of both traditional
aging with treated HIV, the Veterans Aging Cohort Study
HIV-related factors, including CD4 count and viral load, as well
(VACS) index, has also been proposed to measure frailty
as hepatitis C coinfection, liver fibrosis (FIB-4), hemoglobin,
6 • JID • Brothers et al
estimated glomerular filtration rate (eGFR), race, and age. In-
Summary of Factors Associated With Frailty Among
vestigators have considered adding measures to the index, in-
HIV-positive Individuals on Antiretroviral Therapy
cluding inflammatory markers D-dimer and soluble CD14]. As the VACS index is a measure of multisystem deteriora-
Age [, ]HIV-related measures
tion and vulnerability, we included it as a frailty scale. However,
Longer time since diagnosis
the VACS index differs from other frailty measures as it was de-
Lower current CD4 count [,
signed to predict mortality and includes chronological age and
Lower nadir CD4 count
race Most frailty scales do not include age, as they intend
Low CD4/CD8 ratio [
to describe biological age-related changes independent from
Detectable viral load [
chronological age, and most do not include race, because they
Longer duration of HAART ]
instead incorporate markers of individual physical and mental
Protease inhibitor-containing HAART regimen
Further work is needed to determine the best approach to
Hepatitis C coinfection ]
measure frailty in people aging with HIV. It is important to con-
sider the intended use and setting for a frailty scale, whether as a
brief screening tool or as a comprehensive evaluation, for use in
the community, hospital, or long-term care. Some scales that
Kidney disease []
have been used to identify frailty in people with HIV might
Depressive symptoms ,
not be appropriate for those who are very frail or immobile,
Cognitive impairment []
as they include measures of physical performance (eg, walking
speed , or apply exclusion criteria based on disability
Weak upper and lower extremities []
or comorbidities. One study using a modified version of the
History of falls
frailty phenotype scale in an HIV clinic excluded 19% of partic-
ipants because time constraints prevented assessment of grip
Lower education ,
strength and walking speed and another excluded partici-
Current unemployment [
pants requiring an assistive device to walk [
Low income in past year
Abbreviations: BMI, body mass index; HAART, highly active antiretroviral
EPIDEMIOLOGY OF FRAILTY IN HIV INFECTION
therapy; HIV, human immunodeficiency virus.
Before the introduction of HAART in 1996, men in the MACSstudy who seroconverted were 9 times more likely to be identi-fied as frail (via a modified frailty phenotype) during at least 1
[<200 cells/mm3 [], and <100 cells/mm3 []), lower
study visit than men who remained uninfected (13.9% vs 1.5%
nadir CD4 count [CD4/CD8 ratio ≤0.29 [detectable
prevalence) Risk for frailty increased nonlinearly with age
viral load history of AIDS ], and longer time since
and with duration of HIV infection Frailty was also asso-
diagnosis [], as well as hepatitis C coinfection [], low body
ciated with CD4 count <350 cells/mm3, viral load ≥50 000 cop-
mass index (BMI) , ], high BMI [], lipodystrophy [],
ies/mL, and AIDS [
depressive symptoms , 1-year history of multiple falls
With the introduction of HAART, the prevalence of frailty
[], and lower cognitive performance ]. HIV-positive indi-
appeared to decrease. Among MACS participants, frailty de-
viduals who are frail are also more likely to have lower socioe-
creased from 8% in 1994–1995, when <0.1% of participants re-
conomic status, no more than high school education ],
ceived HAART, to 5% in 2000–2005, when almost 70% were on
current unemployment [and income <$10 000 in the
HAART ]. Among participants presenting with AIDS, frailty
prior year ]. Among people who inject drugs, those with ad-
prevalence decreased from 24% to 10% []. However, from
vanced HIV disease (defined as CD4 <350 cells/mm3 and de-
2007–2011, when grip strength was added to the MACS frailty
tectable viral load) are more likely to be frail than uninfected
scale, 25% of all participants were identified as frail during at
individuals, whereas those without advanced HIV disease are
least 1 study visit []. Here the use of different scales compli-
not more likely to be frail ]. Frail HIV-positive individuals
cates comparison of estimates between studies ,
are also more likely to have been on HAART for longer duration
Among individuals on HAART, multiple factors have been
[and on a protease inhibitor-containing HAART regimen
associated with frailty in cross-sectional studies, using different
and less likely to be on a non-nucleoside reverse transcriptase
frailty scales (Table ). Some are traditional HIV measures, in-
inhibitor-containing regimen; this disparity is not explained
cluding lower current CD4 cell count (measured continuously [
by differences in adherence or successful viral suppression
] and categorically, as <500 cells/mm3 [, <350 cells/mm3
[Frail HIV-positive individuals are also more likely than
Frailty in HIV Infection • JID • 7
the nonfrail to have been hospitalized in the past year and to
outcomes To date, knowledge is limited regarding the
have longer hospital stays
prognostic characteristics of frailty in people with HIV. In 1
Also in cross-sectional studies, markers of inflammation (in-
sample of people who inject drugs, having HIV or being frail
terleukin-6, D-dimer, and soluble CD14) are more strongly cor-
was associated with 3-fold higher likelihood of death, whereas
related with VACS index scores than an index comprised only of
both having HIV and being frail increased the risk 7-fold com-
age, CD4 cell count, and viral load [VACS index scores are
pared to those with neither [In the MACS study, the pres-
also associated with upper and lower extremity strength [
ence of frailty prior to HAART initiation decreased time to
and cognitive impairment ]. Although VACS index scores
AIDS or death [. The prevalence of frailty at baseline was
were suggestive of an association with 1-year history of multiple
8%; 36% of people who frail at baseline developed AIDS or
falls in 1 study, this was not statistically significant []. As falls
died, whereas 16% of people who were not frail developed
are a common outcome identified among frail HIV-negative
AIDS or died ].
older adults ], further research is needed to assess whether
Although assessments of outcomes related to frailty in people
the VACS index is measuring frailty or a different but related
with HIV are limited, multiple prospective studies have evaluat-
construct, including some common components.
ed outcomes in relation to the VACS index. Higher VACS index
Two longitudinal analyses of frailty in people with HIV have
scores are associated with all-cause mortality [coronary
been published, both from the MACS cohort. One report in-
heart disease-related mortality [], and fragility fractures,
cluded data from before 2007 ] and the second data from
suggesting that the index might indeed measure frailty as well
2007 to 2011 [. Each report used a different modification
[]. Compared to CD4 count and viral load, VACS index scores
of the frailty phenotype scale (Table which complicates com-
had better predictive ability for mortality among HIV-positive
parisons between the 2 time periods. In both studies, likelihood
individuals with viral load <500 copies/mL and those age ≥50
of presenting as frail at a later study visit was associated with
lower CD4 count and no greater than high school education[Some risk factors for frailty identified in pre-2007
FUTURE DIRECTIONS: FRAILTY AND HIV CARE
data were not replicated in the second analysis (eg, white,non-Hispanic ethnicity [), and other risk factors were as-
While early data have identified the feasibility and usefulness of
sessed in only 1 study. In pre-2007 data, the association between
measuring frailty in people aging with HIV, the implications of
frailty and low CD4 count was identified independently of low
incorporating frailty concepts into HIV care are unknown. The
viral load (<400 copies/mL) and hepatitis B and C coinfection.
ultimate question will be whether recognizing frailty assists in
Participants with high viral load (>50 000 copies/mL) were also
the clinical management of patients with HIV who are frail.
significantly more likely to become frail In the analysis of
Even when immunologically stable, people with HIV accumu-
data from 2007 to 2011, participants with detectable viral loads
late a variety of health problems, and each individual problem
were not more likely to become frail than those with undetect-
likely cannot characterize overall vulnerability. As people with
able viral loads, but participants with depressive symptoms, di-
HIV live longer, many will survive to such an age that they
abetes mellitus, and kidney disease were more likely to become
might be frail in spite of –not because of –the disease. Models
frail [Also in the 2007–2011 data, HIV-positive participants
of care need to adapt to this changing paradigm, and principles
with a history of AIDS had higher odds of becoming frail than
of frailty management may be useful ]. A challenge in the
HIV-negative participants, whereas HIV-positive participants
management of any patient with complex needs is that many
without history of AIDS did not have higher odds [
clinical interventions are intended to help people with only 1
As frailty represents an integrative marker of health and vul-
problem, and such interventions can do harm in people who
nerability, and the severity of frailty can worsen or improve over
have many problems Interdisciplinary assessment and
time [], more longitudinal research is needed. In particular,
care can improve clinical outcomes for people who are frail,
risk factors for frailty among HIV-positive individuals aging
and screening for frailty among patients with complex needs
with high CD4 counts and undetectable viral loads have not
has been found to be both feasible and useful in primary care
been identified. This will be critical as this profile represents
settings []. Future studies should investigate comprehensive as-
many HIV-positive persons currently ageing successfully with
sessments and frailty screening in the delivery of care to people
treated HIV infection [
aging with HIV.
Healthy aging with HIV may be promoted by early interven-
FRAILTY AND HEALTH OUTCOMES IN HIV
tions among those who are at risk for becoming frail. As frailty is
associated with lower CD4 count, and risk appears to declineonce individuals begin HAART ], early antiretroviral treat-
The clinical importance of frailty is often noted as its ability
ment might delay or reduce the severity of frailty. In longitudinal
to describe individuals more vulnerable to adverse health
studies, some older HIV-negative adults show improvement in
8 • JID • Brothers et al
frailty status over time and not simply progressive decline [].
Frailty might be an especially dynamic process in people with
Financial support. This work was supported in part by a Canadian In-
HIV, particularly in younger people with greater physiologic re-
stitutes of Health Research (CIHR) planning grant on ‘HIV/AIDS and co-
serve and greater opportunity to improve ]. However, con-
morbidities', and also by the Fountain Innovation Fund of the QEII Health
tributions of long-term antiretroviral treatment and toxicity to
Sciences Centre Research Foundation. G. G. is supported by ‘Co-morbidityin relation to AIDS' grant agreement (305522), Seventh Framework Pro-
frailty are unknown. Characteristics of frailty and opportunities
gramme. O. T. is supported by a Banting Postdoctoral Fellowship. K. R. is
for intervention should be investigated among the increasing pro-
supported by a CIHR Operating Grant as well as the Dalhousie Medical Re-
portion of treated HIV-positive individuals who demonstrate
search Foundation through the Kathryn Allen Weldon Chain in AlzheimerResearch.
high CD4 counts and undetectable viral loads.
Potential conflicts of interest. J. F. has received consulting fees from
Evidence is also unavailable regarding effective interventions
Theratechnologies, Inc, and has received payment for lectures from Viiv
for HIV-positive people who are already frail. Much of the ev-
Canada, Gilead Canada, and Abbott Canada. With colleagues, K. R. has ap-plied to various Canadian government schemes to commercialize a version
idence for the care of frail HIV-positive people is necessarily
of a frailty index based on a Comprehensive Geriatric Assessment, and a
based on trials performed on younger and fitter people. Al-
company called Videx Canada was incorporated for this purpose. At present
though some medical interventions developed in fit populations
Videx Canada no longer exists. The version of the frailty index presented
are less effective, or even dangerous, in people who are frail, oth-
here was not the one that Videx aimed to commercialize. Videx Canadaplayed no role in the preparation of this manuscript. K. R. was associated
ers can continue to have important benefits. Although some
with Videx Canada but received no funding while it existed. All other au-
treatments provide smaller risk reductions in people who are
thors report no conflicts of interest.
frail, the high absolute risk for poor outcomes with frailty
All authors have submitted the ICMJE Form for Disclosure of Potential
Conflicts of Interest. Conflicts that the editors consider relevant to the con-
might make this smaller benefit worthwhile ]. People aging
tent of the manuscript have been disclosed.
while receiving HAART are also at high risk of polypharmacyand related adverse outcomes, and people who are frail are likely
most vulnerable []. Better understanding of optimal prescrib-ing for frail patients on HAART is needed.
1. Deeks SG, Lewin SR, Havlir DV. The end of AIDS: HIV infection as a
chronic disease. Lancet 2013; 382:1525–33.
2. High KP, Brennan-Ing M, Clifford DB, et al. HIV and aging: state of
knowledge and areas of critical need for research: a report to the NIH
Office of AIDS Research by the HIV and Aging Working Group. J Ac-
quir Immune Defic Syndromes 2012; 60:S1–18.
The increasing life spans of people with HIV reflect enormous
3. Guaraldi G, Orlando G, Zona S, et al. Premature age-related comorbid-
treatment successes and present new challenges related to aging.
ities among HIV-infected persons compared with the general popula-tion. Clin Infect Dis 2011; 53:1120–6.
Although some people with HIV live to older ages with relatively
4. Deeks SG. HIV infection, inflammation, immunosenescence, and aging.
few health problems, others accumulate multiple problems earlier
Annu Rev Med 2011; 62:141–55.
in life. Risk for HANA conditions and other adverse outcomes
5. Fitch KV, Srinivasa S, Abbara S, et al. Noncalcified coronary atheroscle-
rotic plaque and immune activation in HIV-infected women. J Infect
vary significantly between individuals, and are not fully explained
Dis 2013; 208:1737–46.
by age, HIV disease severity, or duration of antiretroviral treat-
6. Justice AC, Freiberg MS, Tracy R, et al. Does an index composed of
ment and toxicity. With the accumulation of multiple health
clinical data reflect effects of inflammation, coagulation, and monocyteactivation on mortality among those aging with HIV? Clin Infect Dis
problems, it is likely that many people aging with HIV may be
2012; 54:984–94.
identified as frail. Emerging data suggest frailty might be a feasible
7. Clegg A, Young J, Iliffe S, Olde Rikkert M, Rockwood K. Frailty in
and useful integrative marker of multisystem vulnerability in peo-
elderly people. Lancet 2013; 381:752–62.
ple aging with HIV. As people with HIV live longer and with
8. Mitnitski A, Song X, Rockwood K. Assessing biological aging: the origin
of deficit accumulation. Biogerontol 2013; 14:709–17.
more complex health and social care needs, the concept of frailty
9. Brothers TD, Rockwood K. Biologic ageing, frailty, and age-
could be useful for identifying vulnerable individuals, for organiz-
related disease in chronic HIV infection. Curr Opin HIV AIDS. 2014
ing care and for comprehensively measuring the impact of illness
May 17 [Epub ahead of print].
10. Onen NF, Overton ET. A review of premature frailty in HIV-infected
and treatment on overall health status.
persons; another manifestation of HIV-related accelerated aging. CurrAging Sci 2011; 4:33–41.
11. Ruiz M, Cefalu C. Frailty syndrome in patients with HIV infection. Clin
Geriatr 2011; 19:46–9.
12. Onen NF, Agbebi A, Shacham E, Stamm KE, Onen AR, Overton ET.
Frailty among HIV-infected persons in an urban outpatient care setting.
We searched Cochrane Library, CINAHL, PubMed, Embase,
J Infect 2009; 59:346–52.
PyschINFO, and Google Scholar using the terms "frail" or
13. Althoff KN, Jacobson LP, Cranston RD, et al. Age, comorbidities, and
"frailty" along with "human immunodeficiency virus" or
AIDS predict a frailty phenotype in men who have sex with men. J Ger-
"HIV." Additional papers were identified from reference lists
ontol A Biol Sci Med Sci 2014; 69:189–98.
14. Guaraldi G, Baraboutis IG. Evolving perspectives on HIV-associated
of retrieved articles, Google Scholar linking of articles citing re-
lipodystrophy syndrome: moving from lipodystrophy to non-infectious
trieved articles, and personal libraries of the authors.
HIV co-morbidities. J Antimicrob Chemother 2009; 64:437–40.
Frailty in HIV Infection • JID • 9
15. Erlandson KM, Allshouse AA, Jankowski CM, et al. Association of
32. Piggott DA, Muzaale AD, Mehta SH, et al. Frailty, HIV infection, and
functional impairment with inflammation and immune activation in
mortality in an aging cohort of injection drug users. PLOS One 2013; 8:
HIV type 1–infected adults receiving effective antiretroviral therapy. J
Infect Dis 2013; 208:249–59.
33. Ianas V, Berg E, Mohler MJ, Wendel C, Klotz SA. Antiretroviral therapy
16. Desai S, Landay A. Early immune senescence in HIV disease. Curr HIV/
protects against frailty in HIV-1 infection. J Int Assoc Provid AIDS Care
AIDS Rep 2010; 7:4–10.
2012; 12:62–6.
17. Desquilbet L, Margolick JB, Fried LP, et al. Relationship between a frail-
34. Pathai S, Gilbert C, Weiss HA, et al. Frailty in HIV-infected adults in
ty-related phenotype and progressive deterioration of the immune sys-
South Africa. J Acquir Immune Defic Syndr 2012; 62:43–51.
tem in HIV-infected men. J Acquir Immune Defic Syndr 2009;
35. Erlandson KM, Allshouse AA, Jankowski CM, et al. Comparison of
functional status instruments in HIV-infected adults on effective anti-
18. Guaraldi G, Zona S, Stentarelli C, et al. Aging with HIV vs HIV sero-
retroviral therapy. HIV Clin Trials 2012; 13:324–34.
conversion at older age: a diverse population with distinct comorbidity
36. Erlandson KM, Allshouse AA, Jankowski CM, et al. Risk factors for falls
profiles. Antivir Ther 2013; 9:14.
in HIV-infected persons. J Acquir Immune Defic Syndr 2012; 61:484–9.
19. Walston J. Frailty-the search for underlying causes. Sci Aging Knowl-
37. Sandkovsky U, Robertson KR, Meza JL, et al. Pilot study of younger and
edge Environ 2004; 2004:pe4.
older HIV-infected adults using traditional and novel functional assess-
20. Mitnitski AB, Mogilner AJ, Rockwood K. Accumulation of deficits
ments. HIV Clin Trials 2013; 14:165–74.
as a proxy measure of aging. Scientific World Journal 2001; 1:
38. Shah K, Hilton TN, Myers L, Pinto JF, Luque AE, Hall WJ. A new frailty
syndrome: central obesity and frailty in older adults with the human im-
21. Collerton J, Martin-Ruiz C, Davies K, et al. Frailty and the role of in-
munodeficiency virus. J Am Geriatr Soc 2012; 60:545–9.
flammation, immunosenescence and cellular ageing in the very old:
39. Ruiz MA, Aguilar E, Sirisha P, Frontini M, Cefalu C. Characteristics of
Cross-sectional findings from the Newcastle 85 study. Mech Ageing
frail patients in a geriatric-HIV program: the experience of an urban ac-
Dev 2012; 133:456–66.
ademic center at one year follow-up. J Am Geriatr Soc 2012; 60:S217–8.
22. Margolick JB, Chopra RK. Relationship between the immune system
40. Talukdar A, Khanra D, Ray S, et al. HIV among the elderly with special
and frailty: Pathogenesis of immune deficiency in HIV infection and
reference to mode of presentation at a tertiary care hospital in Kolkata,
aging. Aging Clin Exp Res 1992; 4:255–7.
India. Trop Doct 2013; 43:100–2.
23. Theou O, Brothers TD, Mitnitski A, Rockwood K. Operationalization of
41. Womack JA, Goulet JL, Gibert C, et al. Physiologic frailty and fragility
frailty using eight scales and comparison of their ability to predict all-
fracture in HIV-infected male veterans. Clin Infect Dis 2013;
cause mortality. J Am Geriatr Soc 2013; 61:1537–51.
24. Fried L, Tangen C, Walston J, et al. Frailty in older adults: evidence for a
42. Justice AC, Modur SP, Tate JP, et al. Predictive accuracyof the Veterans Aging
phenotype. J Gerontol A Biol Sci Med Sci 2001; 56:M146.
Cohort Study index for mortality with HIV infection: a North American
25. Xue QL. The frailty syndrome: definition and natural history. Clin Ger-
cross cohort analysis. J Acquir Immune Defic Syndr 2013; 62:149–63.
iatr Med 2011; 27:1–15.
43. Tate JP, Justice AC, Hughes MD, et al. An internationally generalizable
26. Searle SD, Mitnitski A, Gahbauer EA, Gill TM, Rockwood K. A stan-
risk index for mortality after one year of antiretroviral therapy. AIDS
dard procedure for creating a frailty index. BMC Geriatr 2008; 8:24.
2013; 27:563–72.
27. Theou O, Brothers TD, Pena A, Mitnitski A, Rockwood K. Identifying
44. Adeyemi O, Livak B. Higher Veterans Aging Cohort Study (VACS) index
common characteristics of frailty across seven scales. J Am Geriatr Soc
scores in HIV-positive adults with CD4 counts <200 cells/mm3 despite
2014; 62:901–6.
viral suppression. J Acquir Immune Defic Syndr 2013; 63:e78–81.
28. Kulminski AM, Ukraintseva SV, Kulminskaya IV, Arbeev KG, Land K,
45. Marquine MJ, Umlauf A, Rooney AS, et al. The Veterans Aging Cohort
Yashin AI. Cumulative deficits better characterize susceptibility
Study index is associated with concurrent risk for neurocognitive im-
to death in elderly people than phenotypic frailty: lessons from
pairment. J Acquir Immune Defic Syndr 2014; 65:190–7.
the Cardiovascular Health Study. J Am Geriatr Soc 2008; 56:
46. Oursler K, Tate J, Gill TM, et al. Association of the VACS index with
exercise capacity in HIV-infected adults. AIDS Res Hum Retroviruses
29. Desquilbet L, Jacobson LP, Fried LP, et al. HIV-1 infection is associated
2013; 29:1218–23.
with an earlier occurrence of a phenotype related to frailty. J Gerontol A
47. Mitnitski A, Bao L, Skoog I, Rockwood K. A cross-national study of
Biol Sci Med Sci 2007; 62:1279–86.
transitions in deficit counts in two birth cohorts: implications for mod-
30. Desquilbet L, Jacobson LP, Fried LP, et al. A frailty-related phenotype
eling ageing. Exp Gerontol 2007; 42:241–6.
before HAART initiation as an independent risk factor for AIDS or
48. Justice AC, Tate JP, Freiberg MS, Rodriguez-Barradas MC, Tracy R.
death after HAART among HIV-infected men. J Gerontol A Biol Sci
Reply to Chow et al. Clin Infect Dis 2012; 55:751–2.
Med Sci 2011; 66:1030–8.
49. Greene M, Justice AC, Lampiris HW, Valcour V. Management of
31. Terzian AS, Holman S, Nathwani N, et al. Factors associated with pre-
human immunodeficiency virus infection in advanced age. JAMA
clinical disability and frailty among HIV-infected and HIV-uninfected
women in the era of cART. J Womens Health (Larchmt) 2009;
50. Gleason LJ, Luque A, Shah K. Polypharmacy in the HIV-infected older
adult population. Clin Interv Aging 2013; 8:749–63.
10 • JID • Brothers et al
Source: http://www.airn.ca/uploads/8/6/1/4/86141358/j_infect_dis_-2014-brothers-infdis_jiu258.pdf
THE CODDLING OF THE AMERICAN MIND SOMETHING STRANGE IS happening at America's colleges and universities. A movement is arising, undirected and driven largely by students, to scrub campuses clean of words, ideas, and subjects that might cause discomfort or give offense. Last December, Jeannie Suk wrote in an online article for The New Yorker about law students asking her fellow professors at Harvard not to teach rape law—or, in one case, even use the word violate (as in "that violates the law") lest it cause students distress. In February, Laura Kipnis, a professor at Northwestern University, wrote an essay in The Chronicle of Higher Educationdescribing a new campus politics of sexual paranoia—and was then subjected to a long investigation after students who were offended by the article and by a tweet she'd sent filed Title IX complaints against her. In June, a professor protecting himself with a pseudonym wrote an essay for Vox describing how gingerly he now has to teach. "I'm a Liberal Professor, and My Liberal Students Terrify Me," the headline said. A number of popular comedians, including Chris Rock, have stopped performing on college campuses (see Caitlin Flanagan'sin this month's issue). Jerry Seinfeld and Bill Maher have publicly condemned the oversensitivity of college students, saying too many of them can't take a joke.
Your Guide to Coumadin®/Warfarin Therapy This booklet is based on a product developed by Carla Huber, A.R.N.P., M.S., Cedar Rapids Community Anticoagulation Clinic, Cedar Rapids, Iowa, under Agency for Healthcare Research and Quality (AHRQ) Grant No. 1 U18 HSO15830-01 to Kirkwood Community College. This document is in the public domain and may be used and