Fibrousdysplasia.org
JOURNAL OF BONE AND MINERAL RESEARCH
Volume 12, Number 10, 1997
Blackwell Science, Inc.
1997 American Society for Bone and Mineral Research
Long-Term Effects of Intravenous Pamidronate in
Fibrous Dysplasia of Bone
ROLAND D. CHAPURLAT,1 PIERRE D. DELMAS,1,2 DANIEL LIENS,1 and PIERRE J. MEUNIER1
Fibrous dysplasia of bone (FD) is a rare disorder characterized by proliferation of fibrous tissue in bone marrow
leading to osteolytic lesions. It causes bone pain and fractures. To date the only treatment is orthopedic.
Histological and biochemical similarities between FD and Paget's bone disease related to increased osteoclastic
resorption led us to propose treatment with the bisphosphonate pamidronate. The aim of the study was to assess
the long-term effects of intravenous pamidronate in FD. In this open label phase III study, 20 patients with FD (11
males and 9 females; mean age 31 years) received courses of 180 mg of intravenous pamidronate every 6 months
(60 mg/day during 3 days by infusion). The mean duration of follow-up was 39 months (range 18 – 64). Severity of
bone pain, number of painful skeletal sites per patient, X-rays of all involved areas, serum alkaline phosphatase,
fasting urinary hydroxyproline, and urinary type I collagen C-telopeptide were assessed every 6 months. The
severity of bone pain and the number of painful sites appeared to be significantly reduced. All biochemical markers
of bone remodeling were substantially lowered. We observed a radiographic response in nine patients with refilling
of osteolytic lesions. A mineralization defect proven by bone biopsy was observed in one case. Four patients
sustained bone stress lines, but no fracture occurred. We suggest that intravenous pamidronate alleviates bone
pain, reduces the rate of bone turnover assessed by biochemical markers, and improves radiological lesions of FD.
Few side effects were observed. (J Bone Miner Res 1997;12:1746–1752)
disability. Sarcomatous transformation of FD is rare andoften occurs after radiation therapy.(7)
FIBROUS DYSPLASIA of bone (FD) is a skeletal disorder RadiologicalsignsofFDconsistmainlyoflyticandcystic
characterized by extensive proliferation of fibrous tissue
lesions, with reduction of cortical thickness, and sometimes
in bone marrow, leading to osteolytic lesions, fractures, and
widening of the diaphysis. Radioisotope bone scans usually
deformations.(1) It represents about 2.5% of bone disorders
disclose increased uptake of isotope in affected areas. This
and 7% of benign bone tumors.(2) Initial symptoms most
feature is useful for defining the skeletal distribution of
often present during childhood or adolescence as bone pain
lesions.(8) Computed tomography (CT) and magnetic reso-
and repeated fractures. The other usual clinical findings are
nance imaging (MRI) can be used for differential diagnosis
bone deformity and neurologic compression, especially
with malignancies.(9,10)
when the facial bones or the skull are involved.(3,4) FD may
FD is a congenital disease, due to a somatic activating
be limited to a single bone (monostotic form) or may
mutation of the gene of the a subunit of the G-protein
involve several bones (polyostotic form). Monostotic forms
resulting in a mosaic population of normal and mutant
are often asymptomatic.(5) The McCune-Albright syndrome
tissues,(11) with an increase in cyclic adenosine monophos-
is a polyostotic form of FD associated with melanotic cuta-
phate (cAMP) formation. This activating mutation can be
neous macules and endocrine abnormalities, including pre-
found in bone cells(12,13) and in the endocrine tumors of the
cocious puberty.(6) Recurrent fractures can cause severe
McCune-Albright syndrome.(11,14) There is also an in-
1Department of Rheumatology and Bone Diseases, Hoˆpital Edouard Herriot, Lyon, France.
2Institut National de la Sante´ et de la Recherche Me´dicale (INSERM), Lyon, France.
EFFECTS OF IV PAMIDRONATE
creased expression of the proto-oncogene c-
fos, presumably
TABLE 1. DISTRIBUTION OF BONE LESIONS OF FD
a consequence of raised adenylate cyclase activity in abnor-mal cells.(12) This increased expression of c-
fos appears to
Number of patients
be specific to FD.(12)
Pregnancy has been implicated in exacerbation of FD
perhaps because of estrogen receptors in the fibrous tis-
sue.(15) Bone lesions include collagen fibers randomly dis-
tributed, synthetized by fibroblasts that can originate by
metaplasia of osteogenic cells.(16) These incompletely dif-
ferentiated osteoblasts produce within connective tissue ir-
regular islands of woven bone with no evidence for later
replacement by mature lamellar bone. Osteocalcin has been
discovered in several types of FD cells, confirming their
osteogenic lineage.(17) Increased rates of bone resorption
can be noted and may be due to elevated secretion of
interleukin-6 (IL-6) by bone cells.(18)
To date, orthopedic surgery has been the only treatment
of FD and consists of preventive measures (curettage, bone
grafting, internal fixation of long bones) and management
of fractures.(19) Calcitonin, mithramycin, and etidronatehave been tried in a few cases of FD with poor results.(20,21)Use of antiresorptive drugs has been proposed because ofthe evidence for increased osteoclastic bone resorption,
mine the sites of the disease but not to assess the efficacy of
mediated by the presence of numerous and large osteoclasts
the treatment. There was a total number of 145 sites of FD
at the interface between marrow fibrous areas and bone
in our 20 patients, with a mean of 7.25 per patient (range
surfaces (with similarities with Paget's disease of bone) and
1–25). There were 65 lesions involving limbs, with 14 pa-
by the increase of fasting urinary hydroxyproline.(1,4,6)
tients having one or more sites in the lower limbs (40
We have assessed the long-term effects of intravenous
lesions). Before treatment, 13 patients were suffering from
pamidronate, a second generation bisphosphonate which is
bone pain. Painful sites were sites of FD.
a potent inhibitor of bone resorption, in 20 patients withFD. We have reported preliminary findings on the short-
term effects of pamidronate in nine patients in 1994.(22)
Pamidronate was given by intravenous infusion over 3
days with a total dose of 180 mg/course (60 mg/day), i.e.,
MATERIALS AND METHODS
one course consists of a complete 3-day package. The drug
was administered in normal saline or glucose solution (1l/day), as a 4-h infusion on 3 consecutive days. During the
Twenty patients have been followed up in an open label
study period, patients received supplements of calcium
study design, 9 females and 11 males, for a mean duration
(1000 mg/day) and vitamin D (800 –1200 IU) or D (600 –
of 39 months (range 18 – 64, SD 5 16.72, 65 years follow-
900 IU) to prevent potential vitamin D deficiency and
up) after the first course of treatment. The mean age at
secondary hyperparathyroidism induced by the bisphospho-
diagnosis was 18 (range 1.5– 46). The mean age at onset of
nate. For the two patients who were 13 years old at the
treatment was 31 (range 13– 69); 18 patients were mature
beginning of treatment, the dose of pamidronate was
adults, and 2 were 13 years old at the beginning of treat-
adapted to their weight (1 mg/kg/day). Patients received a
ment. We chose to perform a study without a control group
course of treatment every 6 months, during the first 18
because FD is a very uncommon and heterogeneous dis-
months, and subsequently every 12 months.
ease. No improvement of FD has been experienced by ourpatients before treatment, and for 12 of them the period
Measurement and follow-up
before diagnostic and treatment was over 4 years.
Two patients had monostotic form. The distribution of
Each patient was examined every 6 months. Biochemical
FD lesions in our patients is presented in Table 1. One
measurements were performed, and X-rays of involved sites
woman had McCune-Albright syndrome, with precocious
were taken at each visit.
puberty at age 8 and characteristic melanotic skin macules.
We used a pain scale to assess the severity of bone pain:
Thirteen patients had sustained one or several fractures
0 for no painful site, 1 for low, 2 for moderate, 3 for
before treatment with pamidronate. Pathological confirma-
medium, and 4 for severe. When patients had several pain-
tion of FD was available for eight patients. For the other 12
ful sites, the most painful was chosen to evaluate the effect
patients, FD was diagnosed with radiographs, because of
of treatment. We also assessed the number of painful sites
characteristic lesions. X-rays were taken for each localiza-
per patient before and after each course of treatment. We
tion in all patients, and bone scans were performed in 14
defined the clinical response as follows: complete response
patients at baseline. These bone scans were used to deter-
if the pain intensity dropped from 4, 3, 2, or 1 to 0, with a
CHAPURLAT ET AL.
Evolution of severity of bone
pain with treatment. Comparison of painscores at each visit with baseline values(Wilcoxon match pairs test).
Evolution of the number of
painful localizations with treatment.
Comparison of pain scores at each visitwith baseline values (Wilcoxon matchpairs test).
number of painful localizations which fell to 0; and partial
worsening without any new treatment, among patients who
response if there is a decrease of the intensity of pain or of
present a response.
the number of painful localizations. We defined radio-graphic response as a decrease in the area of one (or
several) lytic lesion(s) and/or as a thickening of bone cortex.
Laboratory tests were performed before treatment and
Biochemical data at each visit were compared with base-
during the follow-up period (every 6 months) for each
line values, expressed in percentage of variation, using the
patient, including serum calcium, phosphate, total alkaline
Wilcoxon matched pairs test. Pain was assessed by compar-
phosphatase (ALP), and fasting urinary excretion of hy-
ing the data at each visit with the baseline values (for the
droxyproline and calcium, by standard laboratory methods
severity using the pain scale and for the number of painful
in our department (colorimetric assays). We also measured,
sites) with the Wilcoxon matched pairs test.
in a subgroup of patients, serum intact parathyroid hor-mone (PTH) by immunochemoluminometric assay (N:28.5 6 11.2 ng/ml), serum 25-hydroxyvitamin D (25(OH)D)
(D and D isomers together) by competitive binding-pro-
Clinical effects
tein assay (N: 28.1 6 11 ng/ml). Urinary peptides of cross-linking domains of collagen I, also called CTX (CrossLaps
Before the first treatment, 13 patients complained of
Osteometer, Copenhagen, Denmark), a sensitive and spe-
bone pain. The mean severity at baseline was 2.8 on our
cific marker of bone resorption,(23) were measured after a
pain scale. Pain severity was significantly reduced (using the
pamidronate course in 10 patients (12 courses). Urine pyr-
Wilcoxon test) after 6, 12, 18, 24, 30, and 36 months (Fig. 1).
idinoline was also measured in seven patients, with an
The mean number of painful sites per patient at baseline
immunoassay (Pyrilinks, Metra Biosystems, Mountain
was 2.9 (range 0 – 4; SD 1.67), corresponding to a total
View, CA, U.S.A.). We defined the biological response as
number of painful localizations of 41 in our 20 patients. The
follows: partial response if serum ALP and/or fasting uri-
number of painful localizations was significantly reduced
nary hydroxyproline decreased at least 30%, and complete
(Wilcoxon test) after 6, 12, 18, 24, and 30 months (Fig. 2).
response if serum ALP and/or fasting urinary hydroxypro-
The clinical response in these 13 patients was complete in 8
line returned to within normal values. We defined the
of them and partial in 5 of them.
relapse as clinical and/or radiological and/or biological
There was a relapse in 8 patients out of 13, but we

EFFECTS OF IV PAMIDRONATE
(A) Before treatment, 1994. (B)
After treatment, 1995. Radiographic as-pect (A) before and (B) after threecourses of pamidronate: filling of a lyticarea.
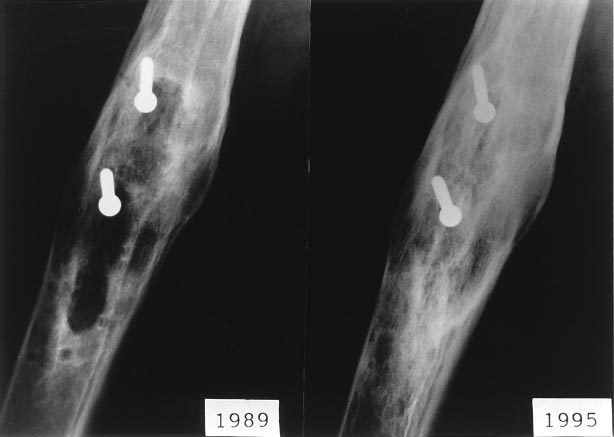
(A) Before treatment, 1989.
(B) After treatment, 1995. Radiographicaspect (A) before and (B) after 10courses of pamidronate: filling of a lyticarea and thickening of a cortice.
obtained a response to a new course of pamidronate in all
on Figs. 3A, 3B, 4A, and 4B. Seven out of the nine patients
of them. Children, the two monostotic patients, and the
who had a radiographic response had painful sites, and all
McCune-Albright patient did not respond differently.
of them presented a clinical response.
No patient sustained a complete fracture. Four patients
developed a stress line during the period of treatment.
These stress lines appeared in a dysplasic area of femur.
Radiological changes were evident in nine patients, con-
Complete healing was achieved for three patients within 6
sisting in a progressive filling of osteolytic areas and in
weeks of ceased weight bearing. For one of these patients
cortical thickening. No obvious changes were observed in
(age 13 at the beginning of treatment), the line has occurred
the other 11 patients. There was neither spreading of pre-
after 7 months of treatment, on a great trochanter, and has
vious lesions nor appearance of new bone lesions during the
increased with time, resulting in a varus of the femoral
period of therapy in all patients. Among these nine patients,
neck. It was necessary to undertake a surgical correction.
two had monostotic FD. A mean of 15 months (range 6 –25)was necessary to achieve a clear improvement in the radio-graphic aspect. The mean age of these patients was 32 years
(range 19 –59 years). There were four females and fivemales. These characteristics were similar to those of the
During the treatment period, repeated infusions of pamidr-
total sample. Examples of radiological changes are shown
onate led to a marked decrease of serum ALP and of urinary
CHAPURLAT ET AL.
TABLE 2. BASELINE VALUES OF BIOCHEMICAL MARKERS
(nmol/mmol Cr)
Data shown are means 6 SD.
intake of calcium. Four patients complained of transientstiffness and bone pain located on the dysplasic areas, whichoccurred once or twice for each of them.
After three courses of pamidronate (540 mg), our
younger patient (age 13 at the beginning of treatment)suffered from unusual changes of the right knee. The thick-ness of the growth plate on the medial side of both thefemur and the tibia expanded over 18 months, reminiscentof rickets. Complete healing of these lesions was observedon X-rays 12 months after cessation of treatment. A trans-iliac bone biopsy in a bone involved by fibrous dysplasiashowed clear evidence of osteomalacia (Fig. 6). A bonebiopsy was also taken in two other adult patients. Focalmineralization defects were seen in these two adult pa-tients, but without increase in the mean osteoid seam widthnor decrease in mean calcification rate measured by bone
Evolution of serum alkaline phosphatase (SAP) as
histomorphometry after tetracycline double labelling.
a function of time, expressed as a percentage of variation.
Comparison of SAP at each visit with baseline values (Wil-
coxon match pairs test).
We provide evidence that in FD treated with intravenous
type I collagen C-telopeptide (CTX). Baseline values of all
pamidronate, bone pain could be alleviated, bone turnover
biochemical markers measured are shown in Table 2.
could be reduced, and radiological lesions could be im-
Serum ALP was significantly lower than baseline values
proved. Few reports have studied the nonsurgical treatment
after 6, 12, 18, 24, 30, 42, and 48 months of treatment
of FD. The existence of increased bone resorption and
(Fig. 5). Urinary CTX levels were reduced after treatment
remodeling activity, at least in agressive forms of FD, en-
by 71%, p 5 0.002, in 10 patients (12 courses).
couraged some open therapeutic trials with calcitonin in
Fasting urinary excretion of hydroxyproline was also de-
order to inhibit osteoclastic resorption. Bell reported a
creased, but this was significant only after 12 and 18
decrease in elevated urinary excretion of hydroxyproline in
months. It was also reduced after 1, 2, and 4 courses of
one patient treated with calcitonin for 16 days.(20) The same
treatment. For the 11 patients in whom it was measured, we
effect was obtained in a 12-year-old girl treated with elca-
observed a trend for a decrease of urinary pyridinoline (not
tonin for 20 weeks.(17) Morii showed a decrease of serum
significant: p 5 0.4).
ALP after administration of porcine calcitonin to a patient
Serum calcium, phosphate, 25 hydroxyvitamin D, and
with polyostotic fibrous dysplasia.(24) But Helmstedt(25) and
fasting urinary excretion of calcium remained unchanged.
Yamamoto(17) did not find any change of serum ALP levels
PTH had a tendency to increase, but this was significant
in their patients treated with calcitonin. No report men-
only after 6 months of treatment (mean 5 74%; p 5 0.038).
tioned the effects of calcitonin on clinical symptoms orX-ray abnormalities. One study reported the effects of atreatment with disodium etidronate(26) in an 18-year-old
Side effects
boy suffering from a polyostotic fibrous dysplasia, who had
We observed some of the side effects usually described
an unsuccessful attempt with calcitonin for 3 months. He
with intravenous pamidronate.(24) Transient fever occurred
has been treated with etidronate 400 mg/day during a 2-
in eight patients after the first infusion (maximum 38.5°C),
week period. This treatment did not induce any change in
but this effect did not reappear with subsequent infusions of
ALP and fasting urinary excretion of hydroxyproline. Be-
pamidronate. Hypocalcemia (minimum: 2.05 mmol/l) was
sides, these parameters were reduced after administration
regularly noted after the infusions, but was seldom symp-
of mithramycin, but this effect lasted only 1 week after the
tomatic (four times) and was quickly corrected by oral
improvement, and this treatment was poorly tolerated.
EFFECTS OF IV PAMIDRONATE
ogeneity of FD. Thus, in the lesions of FD, which wouldcontain too many osteoclasts, fibrous tissue, and/or meta-plasic cartilage in comparison with the amount of osteo-blasts, bone resorption could not be sufficiently inhibited,and the subsequent period of enhanced bone formationwould be inadequate.
The biochemical changes induced by pamidronate in FD
are consistent with a marked reduction of bone remodeling,as shown by the decrease of fasting urinary excretion ofhydroxyproline, and above all of serum ALP and urinaryCTX. Despite the intake of adjuvant calcium and vitaminD, we observed a tendency toward a rise in serum PTH.
This point allows us to emphasize the importance of the
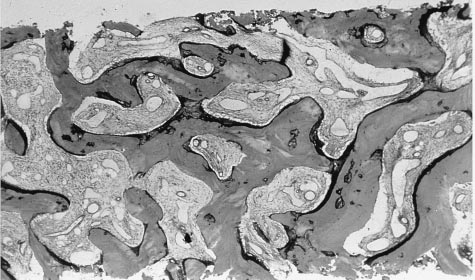
Bone biopsy from the only patient with FD having
adjuvant calcium and vitamin D.
developed a mineralization defect after treatment. Transil-
To improve our knowledge of the disease, biochemical
iac bone biopsy taken in an iliac crest with FD. Osteoma-
markers of bone remodeling should be measured on a
lacia proved by the existence of extended and thick osteoid
monthly basis, at least at the beginning of the follow-up.
seams (in black). Typical fibrosis of marrow spaces also
This would allow the studying of the kinetics of markers
containing many vascular luminae. Undecalcified bone.
after a course of pamidronate on the one hand and of
Goldner method staining. Magnification 503.
whether these kinetics are different among several patientson the other hand. We therefore would be able to decide
Our current study is the continuation of the communica-
more precisely when a new course of treatment is necessary
tion about short-term effects of pamidronate in nine pa-
for one given patient. This moment may be different among
tients with FD.(22) Pamidronate is a potent inhibitor of
different patients because the disease is perhaps more ac-
bone resorption and has, like other bisphosphonates, a
tive in some patients and thus more likely to relapse.
lasting effect on bone turnover.(27) It has been successfully
A transient mineralization defect visible in dysplasic bone
and extensively used in Paget's disease of bone,(28,29) ma-
has occurred in one patient, a 13-year-old boy. In two
lignant hypercalcemia,(30) lytic bone metastases,(31,32) mul-
adults, focal and limited mineralization defects were seen
tiple myeloma,(33) and osteoporosis.(34,35) Intravenous ad-
by biopsy in noninvolved iliac bone. The growth rate of the
ministration is preferred to oral intake because of the poor
adolescent was not affected. The abnormal findings in the
digestive tolerance (gastralgia, esophagitis) of the com-
adolescent may be explained by the increased uptake of
pound when it is given orally(36) and of the low intestinal
pamidronate by his growth plates and by the iliac bone
absorption of bisphosphonates in general.(37) The intrave-
involved with FD. This has very likely increased the focal
nous administration allows a rapid and prolonged intake of
concentration of the compound and enhanced the inhibit-
pamidronate in bone matrix. We chose a dose used in our
ing effects of pamidronate on bone mineralization. Similar
department and by several authors for patients with Paget's
and also reversible changes on growth plates have been
disease of bone.(29)
induced by high daily doses of tiludronate, another bisphos-
In our present study, pamidronate has led to a marked
phonate, in baboons.(38) This fact suggests a cautious use of
decrease in pain severity, and in the number of painful sites
high doses of bisphosphonates in children and the preven-
per patient, as far as an open study permits us to conclude.
tive use of calcium and vitamin D. For these three patients,
Usually two courses of pamidronate were necessary to
it has been possible to resume courses of pamidronate
achieve the improvement. Bone pain was always alleviated
without any problem.
when pamidronate was given after a relapse of bone pain.
In conclusion, intravenous pamidronate appears to have
There was no difference concerning the quality of clinical
potential as a nonsurgical treatment of FD, because it can
response according to the location of the involved sites.
induce radiological and biochemical improvement in some
The radiological survey has shown that in about half of
patients and may alleviate bone pain in most affected indi-
patients lytic lesions could be filled, at least in part, and that
viduals. This treatment was well tolerated, but the possibil-
a thickening of cortices could be obtained. This result is in
ity of a mineralization defect must be monitored in young
agreement with our previous report.(22) Therefore, pamid-
patients. Further double-blind study is required to establish
ronate may induce an increase of bone strength in sites
fully the efficacy of pamidronate for FD.
affected by FD, thus reducing the fracture risk. It must benoted that there are more radiological responses in long
bones of lower limbs than in upper limbs or in skull, but theinterpretation of skull X-rays is far more difficult than for
We thank Dr. M. Arlot for her assistance in statistics and
lower limbs. Furthermore, it is difficult to conclude about
E. Gineyts for the assays of CTX.
the difference of response between lower and upper ex-tremities because we had fewer patients presenting upper
limb involvement. The absence of radiological changes insome patients (or in some sites in patients who show radio-
1. Lichtenstein L, Jaffe
´ HL 1942 Fibrous dysplasia of bone. Arch
logical response) can be explained by the histologic heter-
Pathol 33:777– 816.
CHAPURLAT ET AL.
2. Coley B 1960 Neoplasms of bone and related conditions, Vol 1.
23. Garnero P, Gineyts E, Riou JP, Delmas PD 1994 Assessment
Paul Hocher Inc., New York, NY, U.S.A.
of bone resorption with a new marker of collagen degradation
3. Harris WH, Dudley HR, Barry MD 1962 The natural history of
in patients with metabolic bone disease. J Clin Endocrinol
fibrous dysplasia. J Bone Joint Surg 44A:207–233.
Metab 79:780 –785.
4. Firat D, Stutzman L 1968 Fibrous dysplasia of the bone: Re-
24. Morii H, Tanae A, Ibayashi H, Nakao F 1971 Effects of
view of twenty-four cases. Am J Med 44:421– 429.
calcitonin in metastatic bone carcinoma, osteoporosis, polyos-
5. Henry A 1969 Monostotic fibrous dysplasia. J Bone Joint Surg
totic fibrous dysplasia and hypercalcemia. Endocrinol Jpn
6. Albright F, Butler AM, Hampton AO, Smith P 1937 Syndrome
25. Helmstedt A, Ljunghall S 1979 A case of Albright's syndrome
characterized by osteitis fibrosa disseminata, areas of pigmen-
treated with calcitonin. Acta Orthop Scand 50:251–253.
tation and endocrine dysfunction, with precocious puberty in
26. Long A, Longhlin T, Towers RP, Mc Kenna TJ 1988 Polyos-
females. N Engl J Med 216:727–746.
totic fibrous dysplasia with contrasting response to calcitonin
7. Ruggieri P, Sim FH, Bond JR, Unni KK 1994 Malignancies in
and mythramycin: Aetiological and therapeutic implications.
fibrous dysplasia. Cancer 73:1411–1424.
Int J Med Sci 157:229 –234.
8. Malloy PC, Scott WW, Hruban RH 1993 Case report 769.
27. Fleisch H 1989 Bisphosphonates: A new class of drugs in
Skeletal Radiol 22:66 – 69.
diseases of bone and calcium metabolism. Recent Results Can-
9. Daffner RH, Kirks DR, Gehweiler JA, Heaston DK 1982
cer Res 116:1–28.
Computed tomography of fibrous dysplasia. Am J Roentgen
28. Bijvoet OLM 1991 Disodium pamidronate therapy of Paget's
disease. In: Singer FR, Wallach S (eds.) Paget's Disease of
10. Utz JA, Kransdorf MJ, Jelinek JS, Moser RP, Berrey BH 1989
Bone. Elsevier Science Publishing Co., New York, NY, U.S.A.,
MR appearance of fibrous dysplasia. J Comput Assist Tomogr
pp. 100 –111.
29. Meunier PJ, Vignot E 1995 Therapeutic strategy in Paget's
11. Weinstein LS, Shenker A, Gejman PV, Merino MJ, Friedman
disease of bone. Bone 17:(Suppl):489 – 492.
E, Spiegel MA 1991 Activating mutations of the stimulatory G
30. Ralston SH, Gallagher SJ, Patel U 1989 Comparison of three
protein in the McCune-Albright syndrome. N Engl J Med
intravenous biphosphonates in cancer associated hypercalce-
mia. Lancet 1:1180 –1182.
12. Candeliere GA, Glorieux FH, Prud'homme J, Saint-Arnaud R
31. Van Breukelen FIM, Bijvoet OLM, Van Oosternon AT 1979
1995 Increased expression of the c-fos proto-oncogene in bone
Inhibition of osteolytic bone lesions by (3 amino 1 hydroxypro-
from patients with fibrous dysplasia. N Engl J Med 332:
pylilidene) 1.1 bisphosphonate (APD). Lancet 1:803– 805.
1546 –1551.
32. Burckhardt P, Thie
´baud D, Pery L, Von Fliedner V 1989
13. Malchoff CD, Reardon G, Mc Gillivray DC, Yamase H, Rogol
Treatment of tumor induced osteolysis by APD. Recent Re-
AD, Malchoff DM 1994 An unusual presentation of McCune-
sults Cancer Res 116:54 – 66.
Albright syndrome confirmed by an activating mutation of the
33. Berenson JR, Lichtenstein A, Porter L, Dimopoulos MA, et al.
Gs a-subunit from a bone lesion. J Clin Endocrinol Metab
for the Myeloma Study Group 1996 Efficacy of pamidronate in
¨tsch J, Kiess W, Ha
¨nze J, Repp R, Lu
¨decke D, Blum WF,
reducing skeletal events in patients with advanced multiple
Rascher W 1996 Gsa mutation at codon 201 in pituitary ade-
myeloma. N Engl J Med 334:488 – 493.
noma causing gigantism in a 6-year-old boy with McCune-
34. Reid IR, Wattie DJ, Evans MC, Gamble GD, Stapleton JP,
Albright syndrome. J Clin Endocrinol Metab 81:3839 –3842.
Cornish J 1994 Continuous therapy with pamidronate, a potent
15. Kaplan FS, Fallon MD, Boden SD, Schmidt R, Senoir M,
bisphosphonate, in postmenopausal osteoporosis. J Clin Endo-
Haddad JG 1988 Estrogen receptors in bone in a patient with
crinol Metab 79:1595–1599.
polyostotic fibrous dysplasia (McCune-Albright syndrome).
35. Valkema R, Vismans FJFE, Papapoulos SE, Pauwels EKJ,
N Engl J Med 18:421– 425.
Bijvoet OLM 1989 Maintained improvement in calcium bal-
16. Reed RJ 1963 Fibrous dysplasia of bone: A review of 25 cases.
ance and bone mineral content in patients with osteoporosis
Arch Pathol 75:480 – 495.
treated with the biphosphonate APD. Bone Miner 5:183–192.
17. Yamamoto K, Maeyaa I, Kishimoto M 1983 Suppressive effect
36. Mautalen CA, Casco CA, Gonzalez D, Ghiringhelli GR, Mas-
of elcatonin, an eel calcitonin analogue, on excessive hy-
sironi C 1984 Side effects of disodium aminohydroxypropyli-
droxyproline excretion in polyostotic fibrous dysplasia (Mc-
dene biphosphonate (APD) during treatment of bone diseases.
Cune-Albright's syndrome). Endocrinol Jpn 30:651– 656.
Br Med J 288:828 – 829.
18. Yamamoto T, Ozono K, Kayasama S, Yoh K, Hiroshima K,
37. Fitton A, Mc Tavish D 1991: Pamidronate: A review of its
Takagi M, Matsumoto S, Michigami T, Yamaoka K, Kishimoto
pharmacological properties and therapeutic efficacy in resorp-
T, Okada S 1996 Increased IL-6 production by cells isolated
tive bone disease. Drugs 41:289 –318.
from the fibrous bone dysplasia tissues in patients with Mc-
38. Jiang Y, Zhao J, Van Holsbeeck M 1993 Effects of tiludronate
Cune-Albright syndrome. J Clin Invest 98:30 –35.
on growing bone of baboons: Radiology-pathology correlation.
19. Stephenson RB, London MD, Hankin FM, Kaufert H 1987
Calcif Tissue Int 52(Suppl 2):S46 (abstract 128).
Fibrous dysplasia: an analysis of options for treatment. J Bone
Joint Surg 69A:400 – 409.
20. Bell NH, Avery S, Johnston CC Jr 1970 Effects of calcitonin in
Address reprint requests to:
Paget's disease and polyostotic fibrous dysplasia. J Clin Endo-
Pr. P.J. Meunier
crinol Metab 31:283–290.
Pavillon F
21. Long A, Longhlin T, Towers RP, Mc Kenna TJ 1988 Polyos-
ˆpital Edouard Herriot
totic fibrous dysplasia with contrasting responses to calcitonin
69437, Lyon Cedex 03, France
and mythramycin; aetiological and therapeutic implications.
Int J Med Sci 157(7):229 –234.
22. Liens D, Delmas PD, Meunier PJ 1994 Long-term effects of
Received in original form March 17, 1997; in revised form May 14,
pamidronate in fibrous dysplasia. Lancet 343:953–954.
1997; accepted May 30, 1997.
Source: https://www.fibrousdysplasia.org/wp-content/uploads/2015/12/Chapurlat.LongTermEffectsofIntravenousPamidronateonFibrousDysplasiaofBone.1997.pdf
Revista Alergia México 2014;61(Supl. 2):S117-S193. Guía Mexicana para el Diagnóstico Avalado por Colegio Mexicano de Inmunología Clínica y y el Tratamiento de la Urticaria Presidente: Dr. Miguel Medina Ávalos Colegio Mexicano de Pediatras Especialistas en Inmunología Clínica y Alergia (COMPEDIA) Presidente: José Lozano Saenz
www.digitalfernsehen.de SATELLIT 3 KABEL 3 ANTENNE 22. 5.–24. 5. 2007 Kölnmesse Mit freundlicher Unterstützung: Al e Zeichen stehen auf Erfolg Wenn die Anga ruft, kommt Fachpublikum darf sich über kompetente Referenten auf der pa- ganz Europa. Am 22. Mai rallel stattfindenden Anga Cable Convention freuen. Dass die Mes- ist es wieder so weit. Die se auch in diesem Jahr für die Branche Top-Priorität besitzt, unter-