Scs22637 2114.2117
Hilotherm Efficacy in Controlling Postoperative
Facial Edema in Patients Treated for
Alessandro Moro, MDS, Giulio Gasparini, MDS, Tito Matteo Marianetti, MDS,
Roberto Boniello, DMD, Daniele Cervelli, MDS, Francesco Di Nardo, MD, Francesca Rinaldo, MDS,
Vittoria Alimonti, DMD, and Sandro Pelo, PhD
Background: A cooling system based on polyurethane preshaped
Combined use of glucocorticoids and nonstreoidal anti-
inflammatory drugs is the therapy of choice for edema. In ad-
masks for postoperative cryotherapy, named Hilotherm, has been re-
dition to drug therapies, compression bandages, massage therapy,
cently introduced. The purpose of this study was to evaluate the ef-
and cryotherapy are also used.
fectiveness of this equipment in controlling postoperative edema and
Cryotherapy is the application of ice packs to decrease local
compare the results with those obtained with a group treated with
temperature. This causes vasoconstriction of the precapillary ar-
conventional cryotherapy and a group not treated with cryotherapy.
terioles, decreased tissue perfusion, and diminution of metabolic
Methods: Ninety patients were included in this randomized con-
reactions. Temperature between 12.8-C and 15.6-C is estimated to
trolled trial. The 90 patients were divided into 3 groups. Group A
be most effective in reducing edema.1,2 Cryotherapy administeredby ice packing is definitely an effective antiedemigenic method,
was treated with Hilotherm. Group B was treated with conven-
although it is difficult to quantify its efficacy. Probably, that is the
tional cryotherapy. Group C was not treated with cryotherapy. Using
reason why the protocols used by different authors differ signifi-
a tape measure, we measured for both sides of the face the dis-
cantly in time and mode of administration.
tances in centimeters between point 0 and external canthus (>), most
The main differences are as follows:
lateral point on the ala of the nose (A), commissura labialis (F), and
& freezing mixture (ice, frozen gel, frozen mixture of water and
Pos (C). We performed a Kruskal-Wallis test comparing the aver-
age variation of edema on the right and left sides of the face for
& details of application (whether to place an ice pack directly on
each facial segment of patients of the 3 groups from time 0 to time
& timing of application and duration of treatment
Results: No cryotherapy is the worst treatment for every segment
A new equipment for cryotherapy at constant temperature
studied. In anatomic regions defined A, F, and C, Hilotherm was
(Hilotherm, Argenbu¨hl-Eisenharz, Germany) has recently been in-
more effective in containing edema than the ice pack 24 hours after
troduced. It consists of a polyurethane mask connected to a circuit in
the first measurement. Opposite results were seen on district >, the
which the coolant flows (demineralized water). The masks provided
site not completely enclosed in the mask.
with the device are modeled to fit the different regional anatomies
Conclusions: The substantial difference between different treat-
ments probably consisted in the greater reliability of the Hilotherm
The purpose of this study was to evaluate the effectiveness
system, which is characterized by easy handling, constant temper-
of this equipment in controlling postoperative edema and compare
ature control, comfort, and practicality of the masks.
the results with those obtained with a group treated with conven-tional cryotherapy and a group not treated with cryotherapy.
Key Words: Hilotherm, postoperative swelling, edema,facial edema, postsurgical swelling, cryotherapy, hilotherapy,
MATERIALS AND METHODS
maxillofacial surgery, Le Fort, osteotomy, swelling control
Ninety patients were included in this randomized con-
(J Craniofac Surg 2011;22: 2114Y2117)
trolled trial. Patients were admitted to our institution from April2009 to April 2010. Fifty-eight patients were affected by progenicsyndrome, 30 by prognathism, and 14 by maxillomandibularasymmetry. The sample consisted of 38 women and 52 men agedbetween 19 and 41 years, with an average age of 29 years. These
From the Department of Oral and Maxillofacial Surgery, Columbus Hospital,
patients underwent orthognathic surgery under general anesthesia.
Universita Cattolica del Sacro Cuore, Rome, Italy.
All patients underwent Le Fort I osteotomies + bilateral sagittal
Received November 30, 2010.
split osteotomy of the mandible. The 90 patients were divided into
Accepted for publication January 30, 2011.
3 groups (groups AYC). The 3 groups differed for the method of
Address correspondence and reprint requests to Vittoria Alimonti, DMD,
application of cryotherapy.
Department of Oral and Maxillofacial Surgery, Columbus Hospital,
Group A was treated with Hilotherm, applied in the operat-
Universita Cattolica del Sacro Cuore, 31-33 Giuseppe Moscati,
ing room and maintained for 48 hours. Therapy was periodically
Rome 00168, Italy; E-mail:
[email protected]
interrupted to allow meals and personal hygiene. The cryotherapy
The authors report no conflicts of interest.
protocol with Hilotherm consisted in wearing a mask of polyure-
Copyright * 2011 by Mutaz B. Habal, MDISSN: 1049-2275
thane, preshaped to fit the middle and lower thirds of the face. The
mask was connected by tubes to a portable structure, which makes
The Journal of Craniofacial Surgery & Volume 22, Number 6, November 2011
Copyright 2011 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.

The Journal of Craniofacial Surgery & Volume 22, Number 6, November 2011
Controlling Postoperative Facial Edema
In all groups, no other antiedemigenic aids were used. To
evaluate the efficacy of the therapy with Hilotherm, we measureddistances between defined points on the skin with a tape measure,as described by Laureano et al.2 We stained those points with anindelible marker and used them as landmarks.
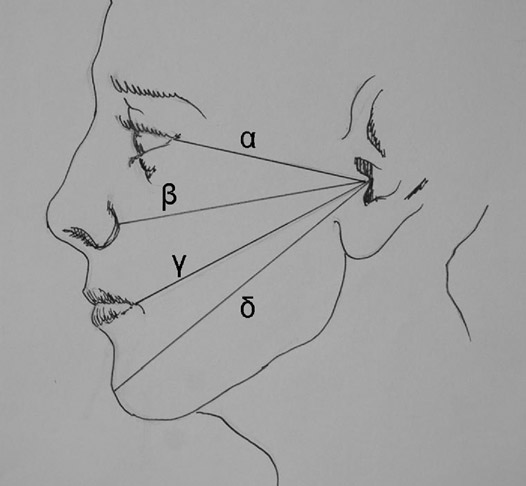
Before surgery, 5 landmarks were marked on each side:
& point 0 (lowest point in the pit between tragus and antitragus)& external canthus& most lateral point on the ala of the nose& commissura labialis& Pos (most prominent point of the chin skin)
Using a tape measure (extension: 1 m, definition: 0.1 cm), we
measured for both sides of the face the distances in centimetersbetween point 0 and& external canthus& most lateral point on the ala of the nose& commissura labialis& Pos
We named the following:
FIGURE 1. A, Hilotherm system. B and C, Application of the
) >: distance between point 0 and the external corner of the eye
polyurethane mask.
) A: distance between point 0 and the most lateral point on the wing
use of demineralized water as coolant. The temperature was ad-
) F: distance between point 0 and the corner of the lips
justable between +10-C and +30-C and was constantly kept at +
) C: distance between point 0 and Pos
15-C. In this study, we exclusively applied the mask model for the
Each measurement was repeated at least 3 times to mini-
middle and lower thirds of the face (Fig. 2).
Group B was treated with conventional cryotherapy, which
mize the operator's errors in detection. Measurements were made
involved local application of ice for 30 minutes every 90 minutes
after 30 minutes, after 24 hours, and after 48 hours from the endof surgery (time 0). Then we calculated the variations of these
during the vigil period, as described by many authors.4 Ice packingstarted within an hour after the end of the surgery and was main-
lengths in centimeters after 24 hours from time 0.
tained for 48 hours.
Finally, we calculated for each patient the average of the sums
Group C was not treated with cryotherapy.
of the values found on the right and left sides of the face for eachfacial segment, and we called these values >1, A1, F1, and C1; for
Surgical procedures were identical in all groups. The sur-
gical team was the same during every surgical intervention. No
example, >1 = (> on the left side + > on the right side) / 2.
complications occurred during surgery and postoperative stage.
Statistical Analysis
Anesthetic procedures were identical in all patients. Titanium plates
To evaluate the differences between the results of the treat-
and screws were used for the rigid fixation of the maxilla; man-
ment with Hilotherm, with ice and without cryotherapy, we per-
dibular fixation was obtained with 3 bicortical screws for each side.
formed a Kruskal-Wallis test comparing the variation of the values
Every patient started soft diet on the morning after surgery.
>1, A1, F1, and C1 of the patients of groups A, B, and C from time
The 3 groups were administered the following medications during
0 to time 24 hours.
the postoperative period:& piperacillin sodium (2085 g) + tazobactam sodium (268.3 mg)
intravenously (IV) every 12 hours for 10 days
& esomeprazole 40 mg IV every 12 hours for 5 days
The average variations in swelling from time 0 to time
& betamethasone 4 mg IV every 12 hours on the first day, 1.5 mg
24 hours of >1 were found to be 0.237 cm in group A (indicating
every 12 hours on the second day, suspended on the third day
an average increase of edema), 0.227 cm in group B, and 0.36 ingroup C; this difference was statistically significant (Kruskal-Wallistest P = 0.002) (Fig. 3).
Average variations in swelling from time 0 to time 24 hours
on A1 were 0.357 cm in group A and 0.62 cm in group B and 0.783in the group C. Significant differences were found (Kruskal-Wallistest P G 0.001) (Fig. 3).
FIGURE 2. Anatomic regions studied. >: externalcanthus-tragus; A: most lateral point on the ala of the
FIGURE 3. Average variation of the swelling on >1, A1, F1,
nose-tragus; F: commissura labialis-tragus; C: pos
and C1 after 24 hours from time 0 in patients treated
(most prominent point of the chin skin-tragus).
with ice versus patients treated with Hilotherm.
* 2011 Mutaz B. Habal, MD
Copyright 2011 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
The Journal of Craniofacial Surgery & Volume 22, Number 6, November 2011
On F1, there was a mean value of 0.457 cm in patients
phology of the patient and restricts the hypothermic effect to the
of group A, a mean value of 0.667 cm in those of group B, and a
areas affected by injury. It also ensures uniform cooling and avoids
mean value of 0.867 cm in patients of group C. The Kruskal-Wallis
abrupt temperature gradients. The mask can be placed directly in the
test confirmed the presence of statistically significant difference
operating room at the end of surgery and constantly worn for several
(Kruskal-Wallis test P G 0.001) (Fig. 3).
days. An element of discomfort is related to the formation of water
As for the comparison of the values of C1, we recorded an
droplets on the polyurethane masks, by condensation of the sur-
average variation of swelling of 0.513 cm in patients of group A, a
rounding air.
mean change of 0.71 cm in group B, and a mean value of 0.873 cm
In our study, we set Hilotherm at 15-C. At this tempera-
in the group C. The Kruskal-Wallis test found statistically significant
ture, we could not detect any damage from hypothermia, but ob-
differences between the 3 treatments on C1 (Kruskal-Wallis test
tained a local analgesic effect. Belli et al10 evaluated comfort in
P G 0.001) (Fig. 3).
using Hilotherm with a questionnaire in a group of 10 patientswho underwent orthognathic surgery. People involved in this
study were asked to assign a score within 0 and 2 to the follow-
Cryotherapy reduces local temperature (between 10-C and
ing parameters: pain, comfort at application, and comfort during
15-C), and it has different effects on postoperative edema:
& decrease of the cellular metabolism that allows the cells to sur-
They stated that therapy with Hilotherm reduced the inten-
vive with less oxygen consumption and less secondary hypoxic
sity and duration of edema and soothed pain. According to these
authors, Hilotherm granted better and faster recovery of mandibu-
& vasoconstriction that reaches its maximum intensity at 15-C7
lar function, greater comfort, and easier patient management by the
& reduction of the microvascular permeability and leakage of
nursing staff.
According to literature, there are various methods of mea-
& decrease of the conduction speed of peripheral motor and sensory
suring edema. These methods include techniques that make use of
nerves that causes reduction of local pain and muscle spasm9
computed tomography scans, magnetic resonance imaging, ultraso-nography, three-dimensional range camera, optical scanners, photo-
The traditional cryotherapy application protocols differ in
graphic support, and individual perceptions of the patient.17,18
timing and types of application. There are several types of freez-
Among the existing procedures, we chose to use direct mea-
ing mixtures: ice packs, ice massage, gel packs, ice chips in a plastic
surement of the distances between landmarks on the skin for the
bag, ice in a wash clot, frozen mixture of alcohol and water, pre-
handiness, lack of cost, and lack of invasiveness of this method. We
packaged chemical ice packs, ice wrapped in a paper towel, and
choose to assess the variation of edema after 24 hours from time
melted ice water through wet towels.10
0 because we noticed that after the surgical intervention, edema is
Some authors suggest applying ice packs directly on the
more important at that time.
skin, whereas other authors propose to apply oil on the skin or
Some of the facial segments studied were completely cov-
a cloth between the skin and the ice pack to prevent injury from
ered by the mask (A, F, C), whereas segment > coincided with
the upper border of the mask. Data provided by the analysis of
Different authors propose a variety of administration tim-
segment > indirectly suggests that cryotherapy with Hilotherm
ings. The most widely used protocol is the ice pack application at
is effective on the regions that are fully enclosed by the mask.
intervals of 10 to 20 minutes for 48 to 72 hours,10 but there is no
The results showed that the shape of the premodeled mask is a
clear evidence about the most effective cryotherapy protocol.1,5,11,12
major determinant of the effectiveness of cryotherapy with Hilo-
Many studies compared the efficacy of intermittent therapy
therm. No cryotherapy is worst treatment for every segment
to continuous therapy, leading to contradictory results.13,14 More-
studied. In anatomic regions defined A, F, and C, 24 hours after the
over, according to the literature, we demonstrated that a treatment
first measurement, Hilotherm was more effective in containing
with cryotherapy is capable of decreasing edema better than a
edema than the ice pack. Opposite results were seen on district
treatment without cryotherapy. Conventional cryotherapy has some
> (joining tragus-external corner of the eye), the site not com-
drawbacks, partly due to the patient, partly due to the method.
pletely enclosed in the mask, where treatment with ice con-
Patients often disregard the intervals of time of applica-
tained swelling in 24 hours better than Hilotherm. Patients treated
tion and cannot continue the application when they sleep (night
with Hilotherm had a reduction in swelling after 24 hours from
interruption). The correct placement of the ice pack is neither
time 0 more than those treated with ice on anatomic regions
controllable nor constant, and patient cooperation might be poor.
Moreover, ice pack cannot provide uniform heat conduction. What
Cryotherapy with Hilotherm has proven an effective anti-
is well known is that rapid changes in temperature and extreme
edemigenic aid, superior to application of ice packs. In this study,
low temperatures should be avoided. It is also apparent that cryo-
the reduction of edema induced by Hilotherm resulted higher than
therapy should start early after injury at temperatures between 10-C
that obtained with other methods.
The substantial difference between different treatments prob-
Patients undergoing conventional cryotherapy might incur
ably consisted in the greater reliability of the Hilotherm system,
different adverse effects: damage from hypothermia,6,9,15 vasodila-
which is characterized by easy handling, constant temperature con-
tation caused by block of nerve conduction, paralysis of the con-
trol, comfort, and practicality of the masks. This allows start-
tractile mechanism of the vascular walls,7,16 and intense perception
ing cryotherapy immediately after surgery, avoiding sudden changes
in temperature, excessive hypothermia, or damage by freezing;
Unlike traditional cryotherapy, therapy with Hilotherm is not
Hilotherm can also be applied regardless of patient's cooperation.
subject to interruptions (possibility to keep the mask during the
Cryotherapy with Hilotherm has proven effective in all anatomic areas
night); it is not affected by the state of consciousness or the co-
included in the mask we used.
operation of the patient and ensures a uniform temperature dis-tribution on the involved soft tissues.
Application temperature can be chosen between 10-C and
1. Greenstein G. Therapeutic efficacy of cold therapy after intraoral
30-C. The preshaped polyurethane mask adapts easily to the mor-
surgical procedures: a literature review. J Periodontol 2007;78:790Y800
* 2011 Mutaz B. Habal, MD
Copyright 2011 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
The Journal of Craniofacial Surgery & Volume 22, Number 6, November 2011
Controlling Postoperative Facial Edema
2. Laureano Filho JR, de Oliveira e Silva ED, Batista CI, et al. The
13. Dolan MG, Thomton RM, Fish DR, et al. Effects of cold water
influence of cryotherapy on reduction of swelling, pain and trismus
immersion on edema formation after blunt injury to the hind limbs
after third-molar extraction. A preliminary study. J Am Dent Assoc
of rats. J Athl Train 1997;32:233Y237
14. McDonald WD, Guthrie JD Jr. Cryotherapy in postoperative setting.
3. Nusair YM. Local application of ice bags did not affect postoperative
J Foot Surg 1985;24:438Y441
facial swelling after oral surgery in rabbits. Br J Oral Maxillofac Surg
15. Sunderland S. Nerve and Nerve Injuries. New York: NY:
Churchill Livingstone, 1978:186Y1 88; further review: Nerve
4. Hochberg J. A randomized prospective study to assess the efficacy
Injuries and Their Repair. 2nd ed. New York, NY: Churchill
of two cold-therapy treatments following carpal tunnel release.
Livingstone, 1991
J Hand Ther 2001;14:208Y215
16. Kanlayanaphotporn R, Janwantanakul P. Comparison of skin
5. Barber F. A comparison of crushed ice and continuous flow cold
surface during the application of various cryotherapy modalities.
therapy. Am J Knee Surg 2000;13:97Y101
Arch Phys Med Rehabil 2005;86:1411Y1415
6. Deal DN, Tipton J, Rosencrance E, et al. Ice reduces edema: a study
17. Knight K. Cryotherapy-Theory, Technique and Physiology.
of microvascular permeability in rats. J Bone Joint Surg Am
1st ed. Chattanooga, TN: Chattanooga Corporation,
7. Guyton AC. Medical Physiology. Philadelphia, PA: WB Saunders Co,
18. Milles M, Desjardins PJ, Pawel HE. The facial plethysmograph:
a new instrument to measure facial swelling volumetrically.
8. Llewelyn J, Ryan M, Santosh C. The use of magnetic resonance
J Oral Maxillofac Surg 1985;43:346Y352
imaging to assess swelling after the removal of third molar teeth.
19. Malone TR, Engelhardt DL, Kirkpatrick JS, et al. Nerve
Br J Oral Maxillofac Surg 1996;34:419Y423
injury in athletes caused by cryotherapy. J Athl Train 1992;27:
9. Stillwell K. Handbook of Physical Medicine and Rehabilitation. 2nd ed.
Philadelphia, PA: WB Saunders, 1971:268Y272
20. La Velle BE, Snyder M. Differential conduction of cold through
10. Belli E, Rendine G, Mazzone N. Cold therapy in maxillofacial surgery.
barriers. J Adv Nurs 1985;10:55Y61
J Craniofac Surg 2009;20:878Y880
21. Taber C Contryman K, Fahrenbruch J, et al. Measurement of reactive
11. Knight KL. Cryotherapy in Sports Injury Management. Champaign, IL:
vasodilatation during cold gel pack application to nontraumatized
Human Kinetics, 1995:95Y98
ankles. Phys Ther 1992;72:294Y299
12. Chotani MA, Flavahan S, Mitra S, et al. Silent >2C adrenergic
22. Lowitzsch K, Hops HC, Gallard J. Changes of sensory conduction
receptors enable cold-induced vasoconstriction in cutaneous arteries.
velocity and refractory periods with decreasing tissue temperature in
Am J Physiol Heart Circ Physiol 2000;278:1075Y1083
man. J Neurol 1977;216:181Y188
* 2011 Mutaz B. Habal, MD
Copyright 2011 Mutaz B. Habal, MD. Unauthorized reproduction of this article is prohibited.
Source: http://hiloterapia.net/wp-content/uploads/Estudio-Mandibluar.pdf
DRAFT FOR CONSULTATION Menopause: diagnosis and management NICE guideline Draft for consultation, June 2015 If you wish to comment on this version of the guideline, please be aware that all the supporting information and evidence is contained in the full version. Menopause: NICE guideline short version DRAFT (June 2015) DRAFT FOR CONSULTATION
Journal of the New Zealand Medical Association Patients admitted with an acute coronary syndrome in New Zealand in 2007: results of a second comprehensive nationwide audit and a comparison with the first audit from 2002 Chris Ellis, Greg Gamble, Andrew Hamer, Michael Williams, Philip Matsis, John Elliott, Gerard Devlin, Mark Richards, Harvey White; for the New Zealand Acute Coronary Syndromes (NZACS) Audit Group