Lichen planus
clinical practice
Laurence Le Cleach, M.D., and Olivier Chosidow, M.D., Ph.D.
This Journal
feature begins with a case vignette highlighting a common clinical problem.
Evidence supporting various strategies is then presented, followed by a review of formal guidelines,
when they exist. The article ends with the authors' clinical recommendations.
A 53-year-old woman presents with intensely itchy skin lesions and burning in her
mouth, which makes eating difficult. These signs and symptoms have become pro-
gressively evident during the past several weeks. Examination of her skin and oral
cavity reveals violaceous, polygonal papules, mainly on the flexural aspect of the
wrists and ankles and in the lumbar region, as well as erosions associated with a lace-
like, white-line network apparent in the posterior buccal mucosa. How should this
case be managed?
The Clinical Problem
Lichen planus is a mucocutaneous inflammatory disease of unknown origin. The skin From the Department of Dermatology,
Hôpital Henri-Mondor, Créteil (L.L.C.,
and oral mucosa are the most frequently involved areas.1 Other mucous membranes O.C.), Université Paris-Est, Créteil Val de
(including the genitalia, esophagus, and conjunctiva) and skin appendages (e.g., scalp Marne (O.C.), and the Centre Cochrane
hair and nails) can also be affected. One or several areas can be involved, either con- Français, Hôpital Hôtel-Dieu, Paris (L.L.C.,
O.C.) — all in France. Address reprint
comitantly or sequentially.2
requests to Dr. Le Cleach at laurence
The clinical presentation of lichen planus varies depending on the area involved3-5
[email protected].
(Fig. 1A through 1F and Table 1). Cutaneous lichen planus is characterized by flat- N Engl J Med 2012;366:723-32.
topped, violaceous papules (Fig. 1A and 1B), the appearance of which may cause
Copyright 2012 Massachusetts Medical Society.
embarrassment1 and which in some cases can be intensely itchy. The lesions may result
in long-standing residual hyperpigmentation, especially in dark-skinned patients.1,6
(Less common variants of cutaneous disease are shown in the figure in the Sup-
plementary Appendix, available with the full text of this article at NEJM.org.) Oral
lichen planus is characterized by symmetric reticular lesions that resemble a white,
lacelike network, as well as by papules, plaques, erythematous lesions, and erosions
(Fig. 1C)7; it is a chronic disease, and its erosive form is painful.3,4 The clinical
An audio version
characteristics of anogenital lichen planus (Fig. 1D and 1E) are typically similar to
of this article
those of both the cutaneous and the oral forms. The erosive form of mucosal lichen
is available at
planus may result in fibrosis, with vulvar scarring, vaginal stenosis,5 phimosis, esoph-
ageal stricture,8 blindness,9 or obstruction of the lachrymal canal. Progressive
scarring can also affect the nails and scalp.10-12
According to population-based data from Sweden, the prevalence of cutaneous
lichen planus among men is 0.3%13 and the prevalence of oral lichen planus is
1.5%14; the respective prevalences among women are 0.1%13 and 2.3%.14 A large study
of patients who presented with oral lesions revealed prior or current cutaneous
lesions in 16% and genital disease in 19%, with rare cases of esophageal, nail, or
conjunctival disease,2 whereas substantially higher rates of concomitant genital or
esophageal disease have been noted on systematic histologic examination in patients
with oral or cutaneous disease.8,15
n engl j med 366;8 nejm.org february 23, 2012
The New England Journal of Medicine
Downloaded from nejm.org by CHAD MILLER on April 16, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
key Clinical points
• Lichen planus is a mucocutaneous inflammatory disease of unknown origin that involves mainly the skin and oral
• The major burdens of lichen planus are itching and residual hyperpigmentation in the cutaneous form and pain and
difficulties with eating in the oral erosive form.
• With the exception of the cutaneous form, which generally heals within 1 year, lichen planus is a chronic condition.
• Given reports of a significant association between lichen planus and infection with the hepatitis C virus (HCV), HCV
serologic testing should be considered in all affected patients.
• In the case of lesions that persist despite treatment, biopsy specimens should be assessed for early dysplasia or
squamous-cell carcinoma, since these conditions have been reported in association with lichen planus.
• Data from randomized, controlled trials are limited, and management choices are based mainly on clinical
• Superpotent topical glucocorticoids are the usual first-line treatment for lichen planus.
Women account for 60 to 75% of patients with the overrepresentation of certain HLA haplotypes
oral lichen planus3,4 and 50% of those with cuta- (e.g., HLA-DR1 in cutaneous lichen planus) sug-
neous lichen planus.6 The mean age at diagnosis gest that genetic factors have a role in susceptibil-
is between 50 and 60 years for oral disease3,4 ity to this disease.1 Several autoimmune disorders,
and between 40 and 45 years for the cutaneous particularly alopecia areata and ulcerative colitis,
form.6 Lichen planus is uncommon in children have been reported to occur more frequently in
(accounting for less than 5% of cases).16
patients with lichen planus than in control popu-
Oral lichen planus is generally considered a lations.21
potentially premalignant condition17; a 1% inci-
There is a significant association between li-
dence of squamous-cell carcinoma has been re- chen planus and infection with hepatitis C virus
ported among patients with this condition in both (HCV). In two meta-analyses, patients with lichen
retrospective and prospective cohort studies.18 planus were reported to be approximately 5 times
However, the true risk remains controversial, as likely as controls to be HCV-seropositive; more-
given the heterogeneous diagnostic criteria for over, lichen planus was 2.5 to 4.5 times as likely
lichen planus across studies (and the difficulty in to develop in the HCV-seropositive patients.22,23
discriminating it from other premalignant condi-
Lichen planus has adverse effects on both
tions), the variation in the duration of follow-up, quality of life and psychological status.24 Factors
and the potential confounding by associated risk that contribute to these detrimental effects include
factors (e.g., alcohol consumption and smok- pain and difficulties with eating and with sexual
ing).4,17,18 Case reports have also described squa- function in association with mucosal disease.
mous-cell carcinomas arising from chronic ano-
genital,5 esophageal,8 or hypertrophic cutaneous
S tr ategies and Ev idence
lichen planus lesions.19
Although the pathogenesis of lichen planus re-
Evaluation and Diagnosis
mains unclear, it appears to be an autoimmune Lichen planus is usually diagnosed clinically. If a
disease. The basal keratinocyte degeneration ob- patient has lichen planus at any site, the clinician
served in lichen planus is attributed to cytotoxic should examine all potentially involved sites, such
CD8+ T lymphocytes,20 which are the major com- as the mucosa, skin, and skin appendages (nails
ponent of the infiltrates located within the epi- [Fig. 1F] and hair [Fig. 1G]). Specialized otorhino-
thelium and adjacent to damaged keratinocytes. laryngologic and endoscopic examinations should
The triggering antigen is not known.20 The exis- be considered when related symptoms such as ody-
tence of rare cases of familial lichen planus and nophagia or dysphagia are present. Differential
n engl j med 366;8 nejm.org february 23, 2012
The New England Journal of Medicine
Downloaded from nejm.org by CHAD MILLER on April 16, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.







clinical practice
Figure 1. Clinical Presentations of Lichen Planus.
Panel A shows widespread eruption of violaceous, shiny, isolated, flat-topped papules and plaques, which are most
profuse on the ankles and in the lumbar region; the legs and neck are also frequently involved. As shown in Panel B,
polygonal, violaceous papules, with a lacelike, white-line network (arrow), are most frequently seen on the inner aspect
of the wrist. Panel C shows the oral lesions of lichen planus, which are bilateral and symmetric and are associated
with a network of white-lined plaques (left arrowhead) and erosive lesions (arrow) in the posterior buccal mucosa
and with a white-line network (right arrowhead) on the top of the tongue. Areas of the oral mucosa mainly affect the
posterior lining of the cheek (in 73% and 91% of cases), the gingiva (33% and 57%), and the tongue (44% and 54%).3,4
Panel D shows a white-line network within an erosive plaque on the glans penis. Panel E shows a white-line network
(arrow) on the internal aspects of the labia minora and majora, which are the sites that are usually affected in anogeni-
tal lichen planus; the vagina is involved in about 50% of cases5 and the perianal area in about 20% of cases.5 Panel F
shows nail thinning, with longitudinal ridging and distal splitting linked to matrix involvement in these two finger-
nails; fingernails are involved more frequently than toenails. Panel G shows follicular, violaceous erythema and acu-
minate keratotic plugs surrounding the zone of alopecia. The plaques are multifocal and occur most frequently on
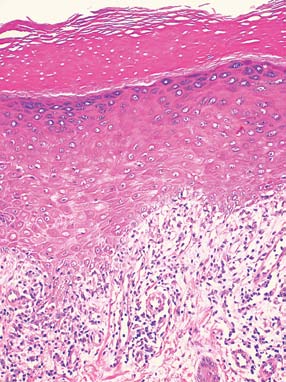
the vertex; other hairy areas can also be involved. The skin specimen in Panel H shows the characteristic histologic
features of lichen planus: thickening of the stratum corneum, with orthokeratosis (thick arrow), accentuation of the
granular-cell layer (thin arrow), liquefactive degeneration of the basal-cell layer (arrowhead), and bandlike inflamma-
tory-cell infiltrate (asterisk) (hematoxylin and eosin).
n engl j med 366;8 nejm.org february 23, 2012
The New England Journal of Medicine
Downloaded from nejm.org by CHAD MILLER on April 16, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
Table 1. Typical Symptoms and Particular Patterns of Lichen Planus, with Possible Outcomes and Complications.
Outcomes and Complications
Koebner's phenomenon: lesion at site
Spontaneous healing, usually within
of traumatic injury (e.g., from
1 yr; long-lasting residual pigmen-
scratching); soles affected more
frequently than palms, with bilater-
al involvement; seen as ery-
thematous scaly plaques, hyperker-
Soreness, pain, burning, swelling, irri-
White forms (reticular, papular,
Poor tendency to heal spontaneously
tation, bleeding; isolated reticular
plaquelike): white, lacelike net-
in about 2.5%3; periods of exac-
form usually asymptomatic
work, papules, plaques; seen in
35%3 and 59%4 of cases; red
forms (erosive, atrophic, bullous):
erythematous lesions with or with-
out erosive lesions associated with
reticular lesions; seen in 41%3 and
Burning, itching, pain, dyspareunia,
Vulvovaginogingival or penogingival
Vulvar scarring in erosive forms (95%
impaired sexual function
syndrome: association between
frequency)5; synechiae with vaginal
erosive genital lichen planus and
stenosis and labia minora aggluti-
nation in females, phimosis in
Odynophagia, dysphagia
Endoscopic findings: stricture mainly
Chronic stricture
located in whitish papules, erythe-
ma, mucosal sloughing
Itching; pain and burning during in-
Frontal fibrosing alopecia: progressive
Chronic and progressive; atrophic,
frontal–temporal hairline recession
scarring alopecia with absence
in postmenopausal women;
of follicular units
syndrome: patchy, scarring alope-
cia associated with follicular li-
chenoid eruption and loss of axil-
lary and pubic hair
Lichen planus of the nail bed leading to
Recovery with treatment, but with fre-
onycholysis and subungual hyperker-
quent relapses; in rare cases, nail loss
or pterygium unguis (permanent
advancement of medial skin over
the nail plate, bisecting the nail)
diagnoses, which vary depending on the clinical treatment in cases of severe disease. Histologic
presentation, are reviewed in Table 1 in the Sup- findings are the same, regardless of the area in-
volved (Fig. 1H). For persistent lesions that do not
Drug-induced lichen planus, also known as li- disappear with treatment, biopsy should be per-
chenoid drug eruption, is uncommon and may be formed to rule out early dysplasia or squamous-cell
indistinguishable from typical idiopathic lichen carcinoma.18
planus25-29 (Table 1 in the Supplementary Appen-
Given the recognized associations between li-
dix). A careful drug history is routinely warrant- chen planus and HCV infection, screening for anti-
ed; in rare cases, drugs that have been taken for as HCV antibodies with the use of an enzyme-linked
long as 2 years before cutaneous lesions develop immunosorbent assay (ELISA) is recommended.
have been considered to be the likely cause of the Some experts believe that for purposes of cost-
effectivenesss, such screening should be reserved
Histologic examination of skin or mucosal bi- for patients known to be at risk for acquiring HCV
opsy specimens is useful to confirm the diagnosis (e.g., intravenous drug abusers),30 whereas other
in atypical cases, as well as to avoid inappropriate experts recommend screening all patients with
n engl j med 366;8 nejm.org february 23, 2012
The New England Journal of Medicine
Downloaded from nejm.org by CHAD MILLER on April 16, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
clinical practice
lichen planus; the choice of screening approach lesion regression or remission at 8 weeks were
should be based on the local seroprevalence of significantly higher with acitretin (30 mg per day
HCV. Routine screening for other immune-mediat- for 8 weeks) than with placebo.33
ed conditions is not thought to be warranted, al-
Another option is phototherapy, although
though these disorders should be considered in this treatment should be used cautiously in dark-
patients with suggestive symptoms or signs.
skinned patients, who have an increased risk of
residual hyperpigmentation. In a small trial involv-
ing 10 patients,34 psoralen and ultraviolet A (PUVA)
Therapeutic objectives depend on the location therapy three times weekly on one side of the body
and severity of the lesions. Since data from ran- was compared with no treatment on the other side
domized, controlled trials are limited,31 treatment of the body. After a mean period of 6 weeks, com-
choices are guided largely by clinical experience. plete clearance (nonpalpable lesions) was noted in
Table 2 summarizes commonly used therapies and half the patients on the treated side only; 2 pa-
their indications. (See Table 2 in the Supplemen- tients with no response had flares while taking
tary Appendix for an expanded list, including thera- the therapy.34 Data from randomized trials of
pies used for nail and scalp lichen planus, as well narrow-band ultraviolet B therapy are lacking. In a
as systemic immunosuppressive therapies.)
retrospective, observational study, 70% of patients
who were treated with narrow-band ultraviolet B
Cutaneous Lichen Planus
therapy had a complete response within a mean of
Because the cutaneous form of lichen planus may 11 weeks.35
resolve spontaneously, the goals of therapy are to
shorten the time between onset and resolution of Oral Lichen Planus
the lesions and to reduce itching. In one study, Reticular oral lichen planus is usually asymptom-
clearing of lesions occurred within 1 year in two atic and does not require treatment.7,17,31 For ero-
thirds of patients with cutaneous disease who were sive oral lichen planus, the goals of treatment are
treated with various regimens.6 Topical glucocorti- to heal erosive lesions and to lessen pain and the
coids are used as the first-line treatment, although associated difficulty in eating and drinking. Topi-
their efficacy has not been demonstrated in well- cal glucocorticoids are the first-line therapy. In two
designed, randomized, controlled trials. Data from small, randomized, placebo-controlled trials —
studies in which various topical glucocorticoids one of fluocinonide36 and the other of betametha-
are compared are lacking. Topical retinoids are not sone valerate37 — the rates of cure or attenuation
prescribed for this condition because of the risk of were significantly higher in the active-treatment
group than in the placebo group (80% with fluo-
When topical glucocorticoids are ineffective, cinonide vs. 30% with placebo, and 66% with
oral glucocorticoid therapy is sometimes used. In betamethasone vs. 18% with placebo).
a small, randomized, controlled trial32 in which
Oral glucocorticoids (e.g., prednisone, at a dose
hydrocortisone 17-butyrate cream alone was com- of 0.5 to 1.0 mg per kilogram of body weight per
pared with oral prednisolone (30 mg per day for day, typically given for 4 to 6 weeks) are generally
10 days) in combination with twice-daily admin- used for erosive lesions that do not respond suffi-
istration of hydrocortisone 17-butyrate cream, sim- ciently to topical glucocorticoids and as first-line
ilar numbers of patients in the two treatment therapy for severe erosive oral lichen planus associ-
groups were reported to have clearing of lesions at ated with eating difficulties. However, data show-
18 weeks, but the time to clearing was signifi- ing the efficacy of this approach are lacking, and
cantly shorter in the group given prednisolone side effects are common. In one randomized tri-
(18 weeks, vs. 29 weeks in the group given the al,38 in which topical triamcinolone was compared
topical cream alone); the limitations of this study with low-dose oral betamethasone (5 mg per day
preclude reliable conclusions.
for 3 months, followed by a slow taper during the
Oral aromatic retinoids are also used. If these ensuing 3 months), the only significant between-
agents are prescribed to women of childbearing group difference was a shorter time to healing in
age, adequate contraception is mandatory (Table the group of patients treated with systemic gluco-
2). In a randomized, controlled trial, the rates of corticoids (15.5 weeks, vs. 19.0 weeks with triam-
n engl j med 366;8 nejm.org february 23, 2012
The New England Journal of Medicine
Downloaded from nejm.org by CHAD MILLER on April 16, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
change maintenance course:
clinical application,
to frequency potent
or controlled different no therapeutic therapy reduce a
diabetes necrosis)
candidiasis; epidermal
features, avascular
Potential
or can temic hypothalamic–pituitary–adrenal cushingoid bone
hibited feeding;
⎫ ⎪ ⎪ ⎪ ⎪ ⎪ ⎬ ⎪ ⎪ ⎪ ⎪ ⎭
thick planus: daily hyper
first-line planus
glucocorticoids,
glucocorticoids:
erosive planus nails: lichen
(without treatment,
topical treatment
atic oral lichen planus: first-line applied
es daily; patient should avoid eating drinking
treatment 3 tim and for treatment ened first-line (under trophic
severe or more ment; resistant second-line
oral plaquelike sions): alone 2
Lichen
for
cinolone acetonide
Commonly
eight/day, for 4 to 6 w
2. Therapies
(e.g., ointment)‡
ral prednisone, 0.5 to 1.0 m
Systemic
n engl j med 366;8 nejm.org february 23, 2012
The New England Journal of Medicine
Downloaded from nejm.org by CHAD MILLER on April 16, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
clinical practice
cinolone), and half the patients had side effects
(twice the rate in the topical-therapy group).
Topical calcineurin inhibitors (cyclosporine,
pimecrolimus, and tacrolimus), although proposed
as possible therapy for this disorder, are not rec-
ommended. They are not approved by the Food and
Drug Administration (FDA) for this indication, and
denotes psoralen and ul
current FDA labeling states that these drugs should
not be given to treat premalignant conditions. A
recent Cochrane review concluded that evidence to
support the contention that topical cyclosporine
women tive datory afterward
reduces pain and clinical signs of oral lichen pla-
nus is weak and unreliable and that there is no
ucosal lichen planus, the severity of the lesions,
evidence to support the notion that pimecrolimus
reduces pain, as compared with topical glucocor-
ticoids or placebo.39
For papular and plaquelike lichen planus with-
be itant erosive m
(but if sessions
out erosive lesions, either topical glucocorticoids
or topical retinoids are used as first-line treatment.
In two small, randomized, placebo-controlled tri-
skin significant cycles of
als in which 0.1% tretinoin lotion was applied for
4 months, twice daily,40 and 0.1% isotretinoin
gel was applied for 8 weeks, twice daily,41 both
the active treatments were superior to placebo.
appear ited increased
Attenuation was observed in 97% of the lotion-
treated patients versus 21% of those given placebo
and in 90% of the gel-treated patients versus
10% of those given placebo. A randomized trial
comparing a topical glucocorticoid (0.1% fluo-
cinolone acetonide) with topical 0.05% retinoic
n expanded version of this table is available in the Supplem
acid for patients with atrophic and erosive oral
second-line with
second-line with
lichen planus showed the former treatment to be
significantly more effective; however, the retinoic
acid concentration was lower than that usually
glucocorticoids a
Anogenital Lichen Planus
For erosive genital lesions, the major therapeutic
cutaneous treatment, glucocorticoids
cutaneous treatment,
ent are described in the text. (A
aim is to prevent or limit scarring. In a prospective
ong second-line therapies should be based on the presence or absence of concom of
cohort study of women with erosive vulvar lichen
planus,5 symptoms were attenuated in 71% of the
women who applied 0.05% clobetasol propionate
ointment (a superpotent topical glucocorticoid)
twice daily, but complete resolution (except for
scarring) was uncommon. Synechiae formation
may be prevented with the use of vaginal dilators
and, for uncircumcised men, foreskin retraction.
When adhesions form, surgery may be required,
but it should be deferred until active lesions are no
longer present in order to avoid complications with
healing. Since lichen planus has been reported to
Systemic
traviolet Gloves Superpotent
* Levels of evidence for specific choices of treatm
† ‡ § For cutaneous lichen planus, the choice am
occur less frequently in circumcised men than in
n engl j med 366;8 nejm.org february 23, 2012
The New England Journal of Medicine
Downloaded from nejm.org by CHAD MILLER on April 16, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
uncircumcised men,43 removal of the foreskin is planus yielded inconsistent results,51,52 so further
study is warranted. It remains unclear how long
maintenance treatment should be continued for
Nail Lichen Planus
mucosal, scalp, nail, and esophageal disease, for
The objectives of treatment in lichen planus of the which there are currently no curative therapies.
nails are to lessen pain and to prevent or limit
scarring. In two retrospective case series, a total of
142 patients were treated with systemic glucocor-
ticoids (intramuscular injection or oral adminis- Guidelines for managing oral lichen planus have
tration), local glucocorticoids (intralesional in- been published by the British Society for Oral
jection or topical application), or both.10,11 Cure Medicine,53 and guidelines for managing vulvar
or major improvement was reported in two thirds lichen planus have been published by the British
of the patients after an average treatment period of Association for Sexual Health and HIV.54 The rec-
6 months; however, relapses were common.
ommendations provided below are generally con-
sistent with these guidelines.
Scalp Lichen PlanusTopical glucocorticoids, either alone or combined
with an intralesional glucocorticoid injection, are
the first-line treatment for lichen planopilaris.12,44
In a retrospective chart review, 20 of 30 patients The woman described in the vignette has oral and
who were treated with topical glucocorticoids cutaneous lesions that appear to be consistent with
(potency level not specified) were found to have a diagnosis of lichen planus. In such patients,
complete clearing of lesions after 12 weeks.45 Li- complete examination of the skin, including the
chen planopilaris that is severe or is resistant to scalp and nails, and of oral, genital, anal, and ocu-
local glucocorticoid therapy is commonly treated lar areas, as well as a thorough gynecologic exami-
with systemic glucocorticoids, although data on nation, should be performed to detect any evidence
the efficacy of this approach are lacking.
of lichen planus elsewhere. Serologic testing for
HCV should be considered. Good oral hygiene
Ar e as of Uncertaint y
should be recommended, and the patient should
be told to avoid cigarette smoking, alcohol con-
It remains uncertain whether, and if so to what sumption, and the ingestion of spicy or acidic foods
extent, lichen planus is an independent risk factor or beverages that can be painful in the presence of
for the development of squamous-cell carcinoma, oral lesions.
as well as whether, and if so how, patients with
We would initiate treatment with topical 0.05%
lichen planus should be monitored for this neo- clobetasol propionate ointment applied three times
plasm.7,17 Randomized trials are needed to pro- daily on erosive areas of the oral mucosa (an ap-
vide better guidance in the choice of the various proach supported by data from randomized trials)
therapies available for the different types of li- and once daily, at night, on involved skin (an ap-
chen planus31,39 and to assess the benefits and proach based largely on clinical experience), with
risks of several medications that have been de- a reevaluation after 6 weeks. If there is no response
scribed to be effective in case reports or small to treatment or if the response is insufficient and
case series. Examples of such medications in- difficulties with eating persist, we would recom-
clude topical rapamycin (now known as sirolim- mend oral glucocorticoids (e.g., prednisone at a
us)46 and extracorporeal photochemotherapy47 dose of 0.5 to 1.0 mg per kilogram per day for 4 to
for erosive oral lichen planus; methotrexate for 6 weeks, followed by a slow taper, to minimize the
cutaneous lichen planus48; a peroxisome prolif- risk of relapse), although data from randomized
erator–activated receptor agonist for lichen pla- trials assessing the efficacy of this therapy or com-
nopilaris49; and anti-CD20 monoclonal antibody paring it with alternative approaches are lacking.
for oral, genital, and esophageal lichen planus.50 If the patient has intense pain or loses weight,
Two randomized, controlled trials comparing aloe systemic rather than topical glucocorticoids can be
vera with placebo for the treatment of oral lichen considered as first-line treatment. Biopsy is war-
n engl j med 366;8 nejm.org february 23, 2012
The New England Journal of Medicine
Downloaded from nejm.org by CHAD MILLER on April 16, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
clinical practice
ranted if healing does not occur with treatment. for attending board meetings from Basilea, consulting fees from
Patients should be educated regarding the poten- Bailleul-Biorga, Pierre Fabre Dermatologie, Astellas, Bayer, and
Galderma, and reimbursement for meeting expenses from
tial side effects of glucocorticoids and should be Basilea and Galderma. No other potential conflict of interest
monitored to detect any such effects. Moreover, relevant to this article was reported.
patients should understand the potentially chronic
Disclosure forms provided by the authors are available with
the full text of this article at NEJM.org.
and relapsing course of oral lichen planus, as well
We thank M. Bigby, B. Gogly, M.M. Landru, J.P. Meningaud,
as the need for long-term clinical surveillance.
and P. Wolkenstein for their helpful comments; B. Cribier,
N. Ortonne, and M. Moyal-Barracco for providing some of the
Dr. Le Cleach reports receiving funds from Abbott and Galderma photographs; and J. Jacobson for editorial assistance on a previ-
for meeting expenses. Dr. Chosidow reports receiving honoraria ous version of the manuscript.
References
1. Pittelkow MR, Daoud MS. Lichen pla-
12. Assouly P, Reygagne P. Lichen plano-
C virus and lichen planus: a reciprocal as-
nus. In: Wolff GK, Goldsmith L, Katz S, pilaris: update on diagnosis and treatment. sociation determined by a meta-analysis.
Gilchrest B, Paller A, eds. Dermatology in Semin Cutan Med Surg 2009;28:3-10.
Arch Dermatol 2009;145:1040-7.
general medicine. 7th ed. New York: Mc- 13. Hellgren L. The prevalence of lichen 24. Tabolli S, Bergamo F, Alessandroni L,
ruber planus in different geographical ar- Di Pietro C, Sampogna F, Abeni D. Qual-
2. Eisen D. The evaluation of cutaneous, eas in Sweden. Acta Derm Venereol 1970; ity of life and psychological problems of
genital, scalp, nail, esophageal, and ocular 50:374-80.
patients with oral mucosal disease in der-
involvement in patients with oral lichen 14. McCartan BE, Healy CM. The report- matological practice. Dermatology 2009;
planus. Oral Surg Oral Med Oral Pathol ed prevalence of oral lichen planus: a re- 218:314-20.
Oral Radiol Endod 1999;88:431-6.
view and critique. J Oral Pathol Med 2008; 25. Halevy S, Shai A. Lichenoid drug
3. Carbone M, Arduino PG, Carrozzo M, 37:447-53.
eruptions. J Am Acad Dermatol 1993;29:
et al. Course of oral lichen planus: a retro- 15. Belfiore P, Di Fede O, Cabibi D, et al. 249-55.
spective study of 808 northern Italian pa- Prevalence of vulval lichen planus in a co- 26. Usman A, Kimyai-Asadi A, Stiller MJ,
tients. Oral Dis 2009;15:235-43.
hort of women with oral lichen planus: an Alam M. Lichenoid eruption following
4. Bermejo-Fenoll A, Sánchez-Siles M, interdisciplinary study. Br J Dermatol hepatitis B vaccination: first North Amer-
López-Jornet P, Camacho-Alonso F, Salazar- 2006;155:994-8.
ican case report. Pediatr Dermatol 2001;
Sánchez N. A retrospective clinicopatho- 16. Walton KE, Bowers EV, Drolet BA, 18:123-6.
logical study of 550 patients with oral li- Holland KE. Childhood lichen planus: de- 27. Kuraishi N, Nagai Y, Hasegawa M,
chen planus in south-eastern Spain. J Oral mographics of a U.S. population. Pediatr Ishikawa O. Lichenoid drug eruption with
Pathol Med 2010;39:491-6.
palmoplantar hyperkeratosis due to ima-
5. Cooper SM, Wojnarowska F. Influ-
17. Lodi G, Scully C, Carrozzo M, tinib mesylate: a case report and a review
ence of treatment of erosive lichen planus Griffiths M, Sugerman PB, Thongprasom of the literature. Acta Derm Venereol
of the vulva on its prognosis. Arch Der- K. Current controversies in oral lichen 2010;90:73-6.
planus: report of an international consen- 28. Asarch A, Gottlieb AB, Lee J, et al. Li-
6. Irvine C, Irvine F, Champion RH. sus meeting. Part 2. Clinical management chen planus-like eruptions: an emerging
Long-term follow-up of lichen planus. and malignant transformation. Oral Surg side effect of tumor necrosis factor-alpha
Acta Derm Venereol 1991;71:242-4.
Oral Med Oral Pathol Oral Radiol Endod antagonists. J Am Acad Dermatol 2009;61:
7. Al-Hashimi I, Schifter M, Lockhart 2005;100:164-78.
PB, et al. Oral lichen planus and oral li- 18. Warnakulasuriya S, Kovacevic T, Mad- 29. Issa Y, Brunton PA, Glenny AM, Dux-
chenoid lesions: diagnostic and therapeu- den P, et al. Factors predicting malignant bury AJ. Healing of oral lichenoid lesions
tic considerations. Oral Surg Oral Med transformation in oral potentially malig- after replacing amalgam restorations: a
Oral Pathol Oral Radiol Endod 2007;103: nant disorders among patients accrued systematic review. Oral Surg Oral Med
over a 10-year period in South East Eng- Oral Pathol Oral Radiol Endod 2004;98:
8. Quispel R, van Boxel OS, Schipper land. J Oral Pathol Med 2011;40:677-83.
ME, et al. High prevalence of esophageal 19. Singh SK, Saikia UN, Ajith C, Kumar 30. Bigby M. The relationship between li-
involvement in lichen planus: a study us- B. Squamous cell carcinoma arising from chen planus and hepatitis C clarified.
ing magnification chromoendoscopy. En- hypertrophic lichen planus. J Eur Acad Arch Dermatol 2009;145:1048-50.
Dermatol Venereol 2006;20:745-6.
31. Le Cleach L, Chosidow O, Cribier B.
9. Brewer JD, Ekdawi NS, Torgerson RR, 20. Sugerman PB, Savage NW, Walsh LJ, et Lichen planus. In: Williams H, Bigby M,
et al. Lichen planus and cicatricial con- al. The pathogenesis of oral lichen planus. Diepgen T, Herxheimer A, Naldi L, Rzany
junctivitis: disease course and response to Crit Rev Oral Biol Med 2002;13:350-65.
B, eds. Evidence-based dermatology. 2nd
therapy of 11 patients. J Eur Acad Derma- 21. Gruppo Italiano Studi Epidemiologici ed. Oxford, England: Blackwell, 2008:189-
tol Venereol 2011;25:100-4.
in Dermatologia. Epidemiological evi- 96.
10. Piraccini BM, Saccani E, Starace M, dence of the association between lichen 32. Kellett JK, Ead RD. Treatment of lichen
Balestri R, Tosti A. Nail lichen planus: re- planus and two immune-related diseases: planus with a short course of oral pred-
sponse to treatment and long term follow- alopecia areata and ulcerative colitis. nisolone. Br J Dermatol 1990;123:550-1.
up. Eur J Dermatol 2010;20:489-96.
Arch Dermatol 1991;127:688-91.
33. Laurberg G, Geiger JM, Hjorth N, et
11. Goettmann S, Zaraa I, Moulonguet I. 22. Lodi G, Pellicano R, Carrozzo M. al. Treatment of lichen planus with acitre-
Nail lichen planus: epidemiological, clini- Hepatitis C virus infection and lichen pla- tin: a double blind, placebo-controlled
cal, pathological, therapeutic and progno- nus: a systematic review with meta-analy- study in 65 patients. J Am Acad Dermatol
sis study of 67 cases. J Eur Acad Dermatol sis. Oral Dis 2010;16:601-12.
Venereol 2011 November 3 (Epub ahead of 23. Shengyuan L, Songpo Y, Wen W, 34. Gonzalez E, Momtaze-T K, Freedman
Wenjing T, Haitao Z, Binyou W. Hepatitis S. Bilateral comparison of generalized li-
n engl j med 366;8 nejm.org february 23, 2012
The New England Journal of Medicine
Downloaded from nejm.org by CHAD MILLER on April 16, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
clinical practice
chen planus treated with psoralens and clinical evaluation. Ann Dermatol Vene- S, Saricaoglu H. Methotrexate for the
ultraviolet A. J Am Acad Dermatol 1984; reol 1994;121:459-63. (In French.)
treatment of generalized lichen planus.
41. Giustina TA, Stewart JCB, Ellis CN, et J Am Acad Dermatol 2009;60:164-6.
35. Pavlotsky F, Nathansohn N, Kriger G, al. Topical application of isotretinoin gel 49. Mirmirani P, Karnik P. Lichen plano-
Shpiro D, Trau H. Ultraviolet-B treatment improves oral lichen planus: a double- pilaris treated with a peroxisome prolifer-
for cutaneous lichen planus: our experi- blind study. Arch Dermatol 1986;122:534- ator-activated receptor gamma agonist.
ence with 50 patients. Photodermatol 6.
Arch Dermatol 2009;145:1363-6.
Photoimmunol Photomed 2008;24:83-6.
42. Buajeeb W, Kraivaphan P, Pobrurksa 50. Parmentier L, Bron BA, Prins C, Sam-
36. Voûte AB, Schulten EA, Langendjik C. Efficacy of topical retinoic acid com-
son J, Masouyé I, Borradori L. Mucocuta-
PNJ, Kostense PJ, van der Waal I. Fluoci- pared with topical fluocinolone acetonide neous lichen planus with esophageal in-
nonide in an adhesive base for the treat- in the treatment of oral lichen planus. volvement: successful treatment with an
ment of oral lichen planus: a double- Oral Surg Oral Med Oral Pathol Oral Ra- anti-CD20 monoclonal antibody. Arch
blind, placebo-controlled clinical study. diol Endod 1997;83:21-5.
Oral Surg Oral Med Oral Pathol 1993;75: 43. Mallon E, Hawkins D, Dinneen M, et 51. Salazar-Sánchez N, López-Jornet P,
al. Circumcision and genital dermatoses. Camacho-Alonso F, Sánchez-Siles M. Ef-
37. Tyldesley WR, Harding SM. Beta-
Arch Dermatol 2000;136:350-4.
ficacy of topical aloe vera in patients with
methasone valerate aerosol in the treat- 44. Sperling LC, Nguyen JV. Treatment of oral lichen planus: a randomized double-
ment of oral lichen planus. Br J Dermatol lichen planopilaris: some progress, but a blind study. J Oral Pathol Med 2010;39:
long way to go. J Am Acad Dermatol 2010; 735-40.
38. Malhotra AK, Khaitan BK, Sethuraman 62:398-401.
52. Choonhakarn C, Busaracome P, Sri-
G, Sharma VK. Betamethasone oral mini- 45. Chieregato C, Zini A, Barba A, Mag- panidkulchai B, Sarakarn P. The efficacy
pulse therapy compared with topical tri- nanini M, Rosina P. Lichen planopilaris: of aloe vera gel in the treatment of oral
amcinolone acetonide (0.1%) paste in oral report of 30 cases and review of the litera- lichen planus: a randomized controlled
lichen planus: a randomized comparative ture. Int J Dermatol 2003;42:342-5.
trial. Br J Dermatol 2008;158:573-7.
study. J Am Acad Dermatol 2008;58:596- 46. Soria A, Agbo-Godeau S, Taïeb A, 53. The British Society for Oral Medicine.
Francès C. Treatment of refractory oral Guidelines for the management of oral
39. Thongprasom K, Carrozzo M, Furness erosive lichen planus with topical rapamy-
lichen planus in secondary care, 2010
S, Lodi G. Interventions for treating oral cin: 7 cases. Dermatology 2009;218:22-5.
lichen planus. Cochrane Database Syst 47. Guyot AD, Farhi D, Ingen-Housz-Oro 54. UK guideline on the management of
S, et al. Treatment of refractory erosive oral vulval conditions. London: British Asso-
40. Boisnic S, Branchet MC, Pascal F, Ben lichen planus with extracorporeal photo-
ciation for Sexual Health and HIV, 2011
Slama L, Rostin M, Szpirglas H. Topical chemotherapy: 12 cases. Br J Dermatol (http://www.bashh.org/guidelines).
tretinoin in the treatment of lichen planus 2007;156:553-6.
Copyright 2012 Massachusetts Medical Society.
and leukoplakia of the mouth mucosa: a 48. Turan H, Baskan EB, Tunali S, Yazici
clinical trial registration
The Journal requires investigators to register their clinical trials
in a public trials registry. The members of the International Committee
of Medical Journal Editors (ICMJE) will consider most reports of clinical
trials for publication only if the trials have been registered.
Current information on requirements and appropriate registries
is available at www.icmje.org/faq_clinical.html.
n engl j med 366;8 nejm.org february 23, 2012
The New England Journal of Medicine
Downloaded from nejm.org by CHAD MILLER on April 16, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
Source: http://remedy.tcs.tulane.edu/portal/files/open-access/Clerkships/internal-medicine/Ambulatory/Lichen_Planus.pdf
British Journal of Nutrition (2007), 98, Suppl. 1, S46–S53 q The Authors 2007 Polyunsaturated fatty acids in the pathogenesis and treatment ofmultiple sclerosis Laurence S. Harbige1,2* and Mohammad K. Sharief 31Centre for Bioscience Research, School of Science, University of Greenwich at Medway, United Kingdom2Medway School of Pharmacy,University of Kent and University of Greenwich, United Kingdom3Department of Neurology, King's, Guy's and St Thomas' Hospital, London, United Kingdom
Réanimation 14 (2005) 621–628 Complications infectieuses des maladies systémiques Infections in systemic rheumatic diseases M. Michel , B. Godeau Service de médecine interne, CHU hôpital Henri-Mondor, 51, avenue du Maréchal-de-Lattre-de-Tassigny, 94010 Créteil cedex, France Malgré les nombreux progrès réalisés dans la prise en charge des maladies systémiques (MS) au cours de la dernière décennie, les compli-